project04:P2
P2
The Academic Medical Center(AMC) is one of the largest hospitals in the Netherlands. The AMC is among the top medical centers in the world. The building dates back to the eighties of the last century. Up until now various architectural interventions have been made but the currently the quality of the building is right on the acceptable level. To maintain an acceptable quality of the building renovation and transformation is required. Therefor the AMC building has to be renewed to face the future. Designing new state of the art medical facilities as for creating a sustainble hospital with a neutral carbon footprint. Within the Architectural Enigineering graduation track this challenge is explored. This is the second presentation in the graduation track presenting my proposal for the new AMC based on Robotic Building principles.
The Academic Medical Center
The AMC's occupation dates back to eighties, The building, well rather the city like complex, has been subjected to aging and intensive usages. But still functions well due to the well integrated design principles of flexibility and oversizing. Even though the building still functions well, the quality of the spaces has fallen to just an acceptable level. Small transformations have been made to improve fragments of the city, while a large scale renovation remains to happen. Meanwhile advancements in the field of medicine are changing the requirements for hospital architecture and the way we use them. In order to adapt to these changing needs I propose the transformation of the complex.
Key figures
Completed:
Floorspace:
Clinical admissions:
Day care admissions:
Outpatient visits:
Beds:
Employees:
Medical students:
Medical informatics students:
1983.
500.000m2
25.000 per year.
30.000 per year.
356.000 per year.
1.002.
7.000.
2.200.
100.
Impression
The Academic medical center has a very recognizable architectural appearance. The building shows of the characteristics of the brutalist architecture style. It is the block like structure and their exposed concrete materialization that support the style. the large scale of the building complex can be clearly seen from the bird's eye perspective building. While other photos show the interior quality of the existing structure where the various buildings form the interior public space. This fits in really well with the brutalistic idea where modular elements from distinct masses and functional zones. While consequently forming a unified whole. But it is these qualities that also provide one of the hospitals problems. The building feels cold and discomforting, especially for the ill.
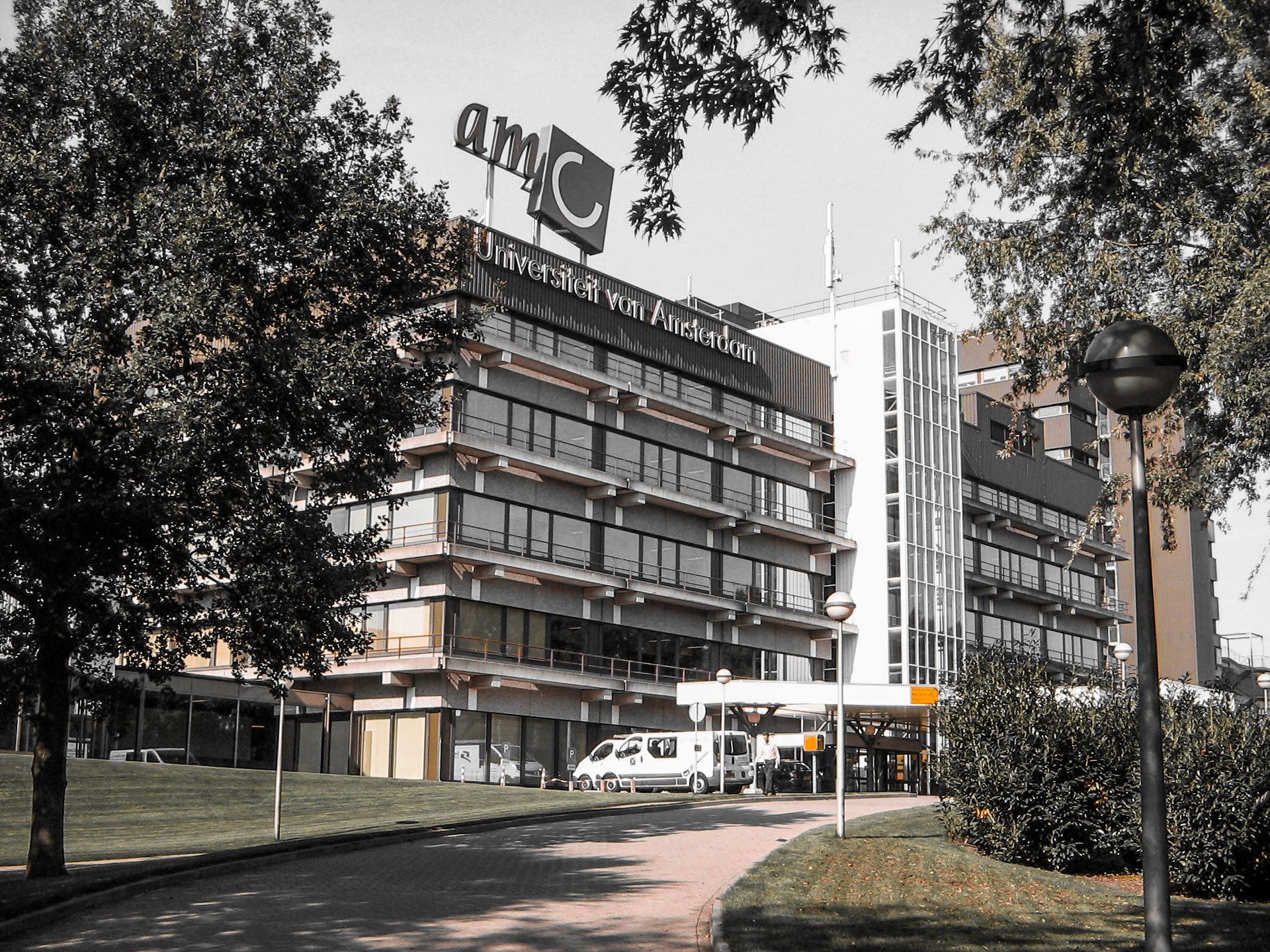





Various images of the AMC.
retrieved from AMC website.
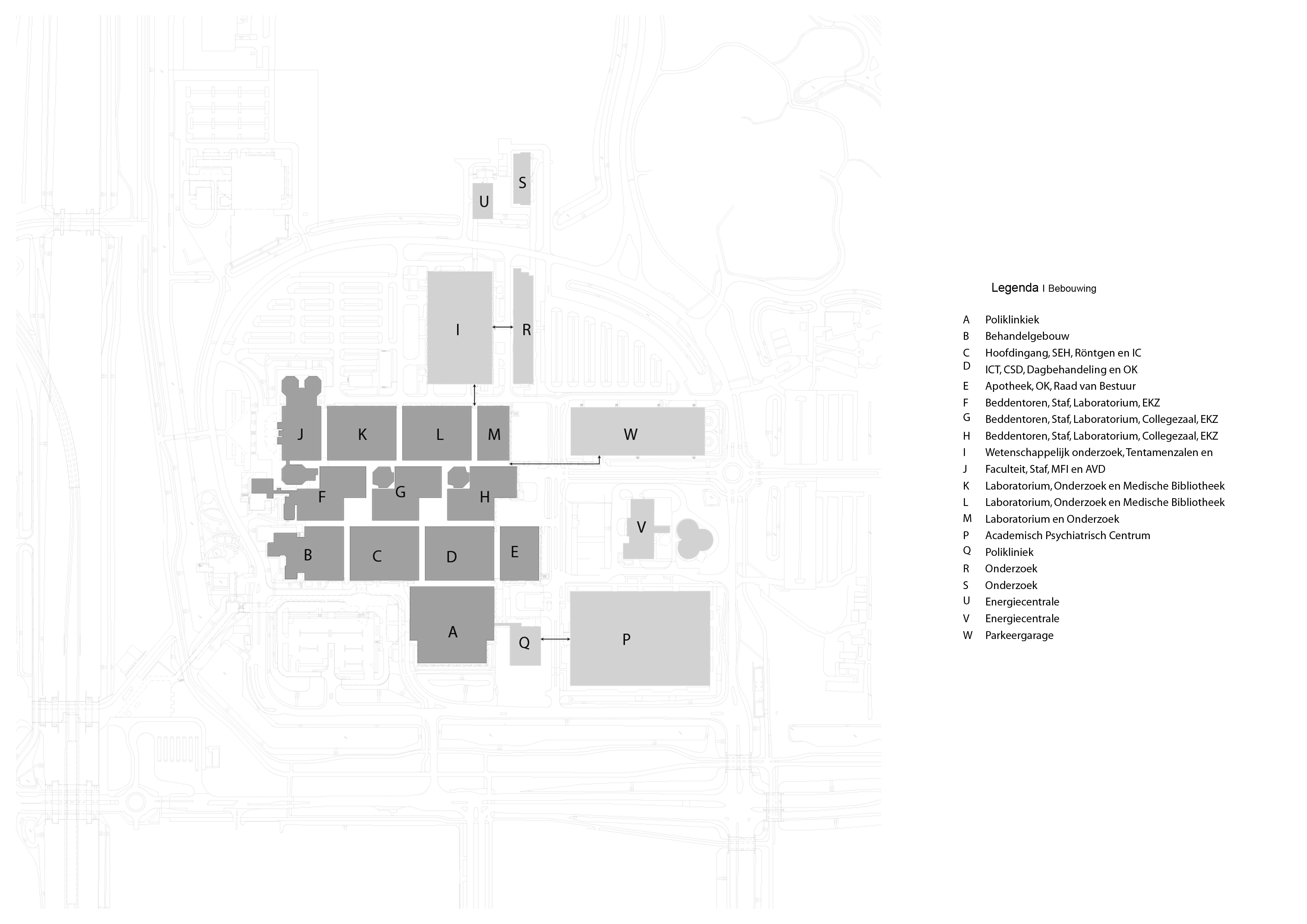
Location
The decision to build this complex dates back to the merging of two hospital with outdated facilities in the city center of Amsterdam. In order to enable future expansion the new building site had been located out of the city center with improved infrastructural access. Over the years the AMC has expended on its plot in order to accommodate more hospital and healthcare function. In the meantime the city of Amsterdam has expanded around the AMC site. Currently the AMC is accessible by the highway network's A2 and A9 and accessible by public transport through Amsterdam Holendrecht station.

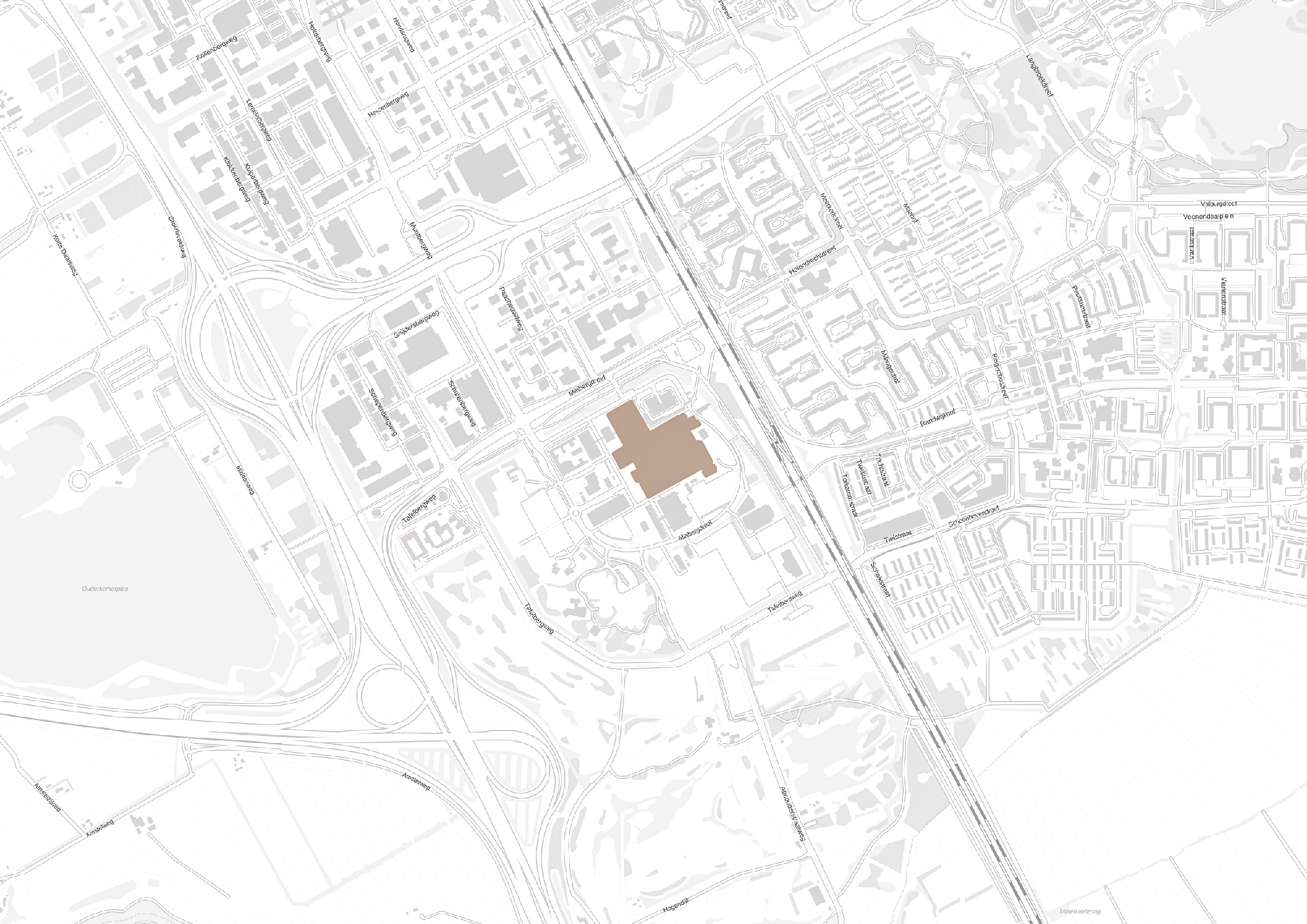
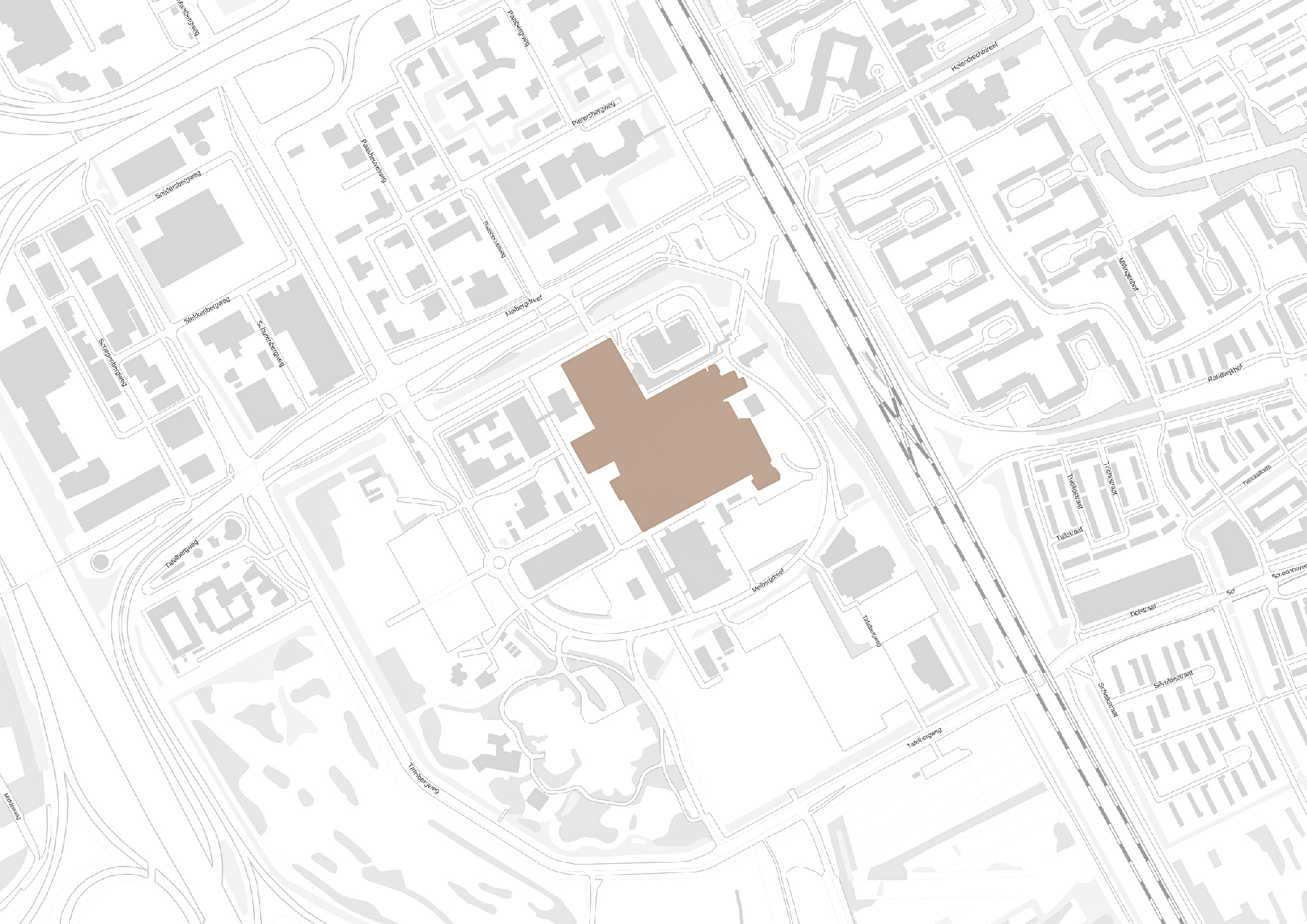
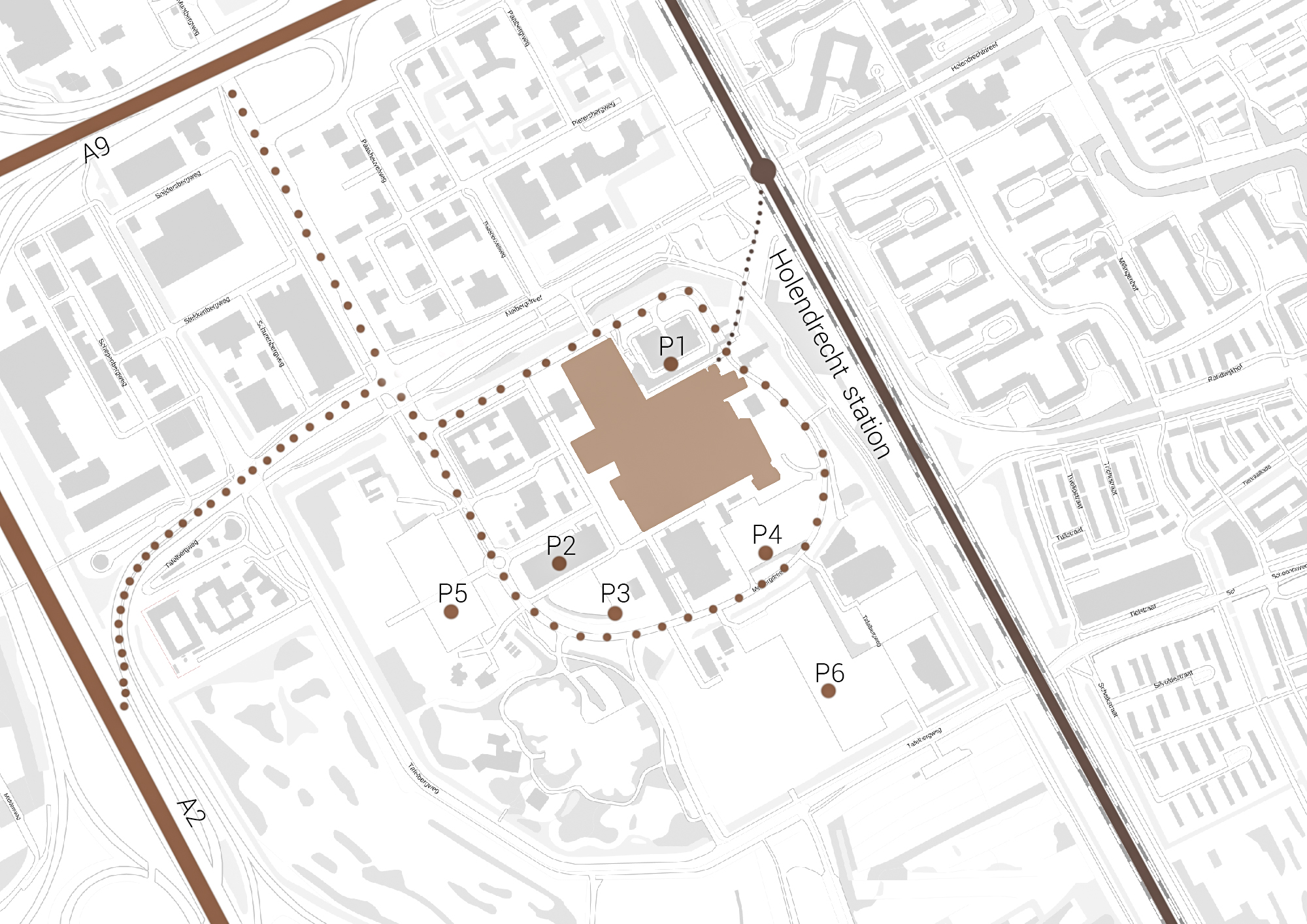
Own images showing the location of the AMC and the access to the building by car and public transport
Floorplans
The various floorplans of the AMC are shown below with their colour corresponding to the their respective functions. The brutalistic function distribution is clearly shown. Most function have their own floor in their own building. One of the other things that these floorplans show is there is a distinct division between north and south. The northern part has been reservered for the functions that are non patient related like education and laboratories whil the southern part is meant for patient care. There is also a division in elevation where the higher floors house the nurseries and patient care units and the lower floor houses public and semi public functions like shops and lecture halls. But one of the drawbacks of this distribution is that it does not place its patient central. While this should be where a hospital should revolve around.
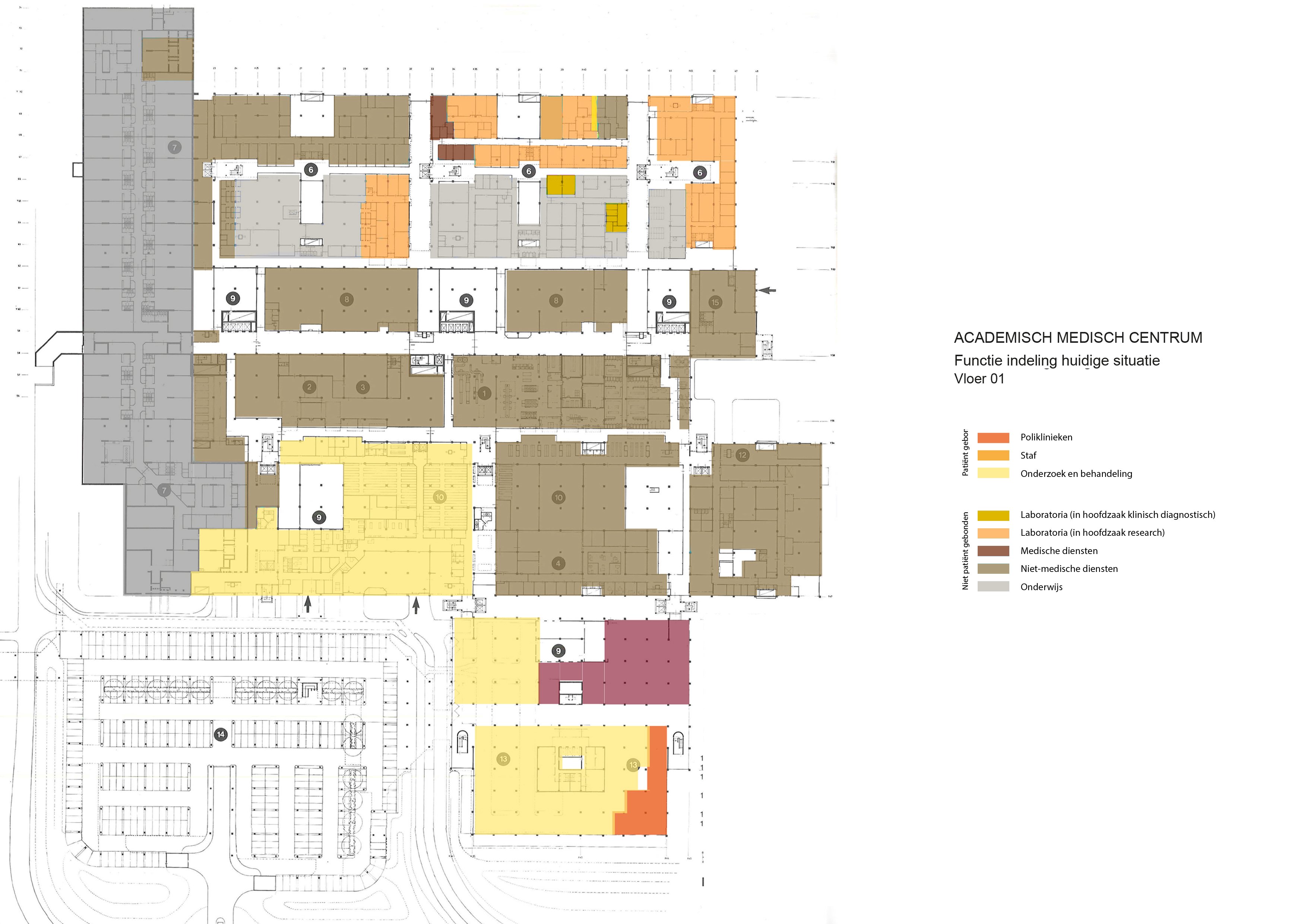
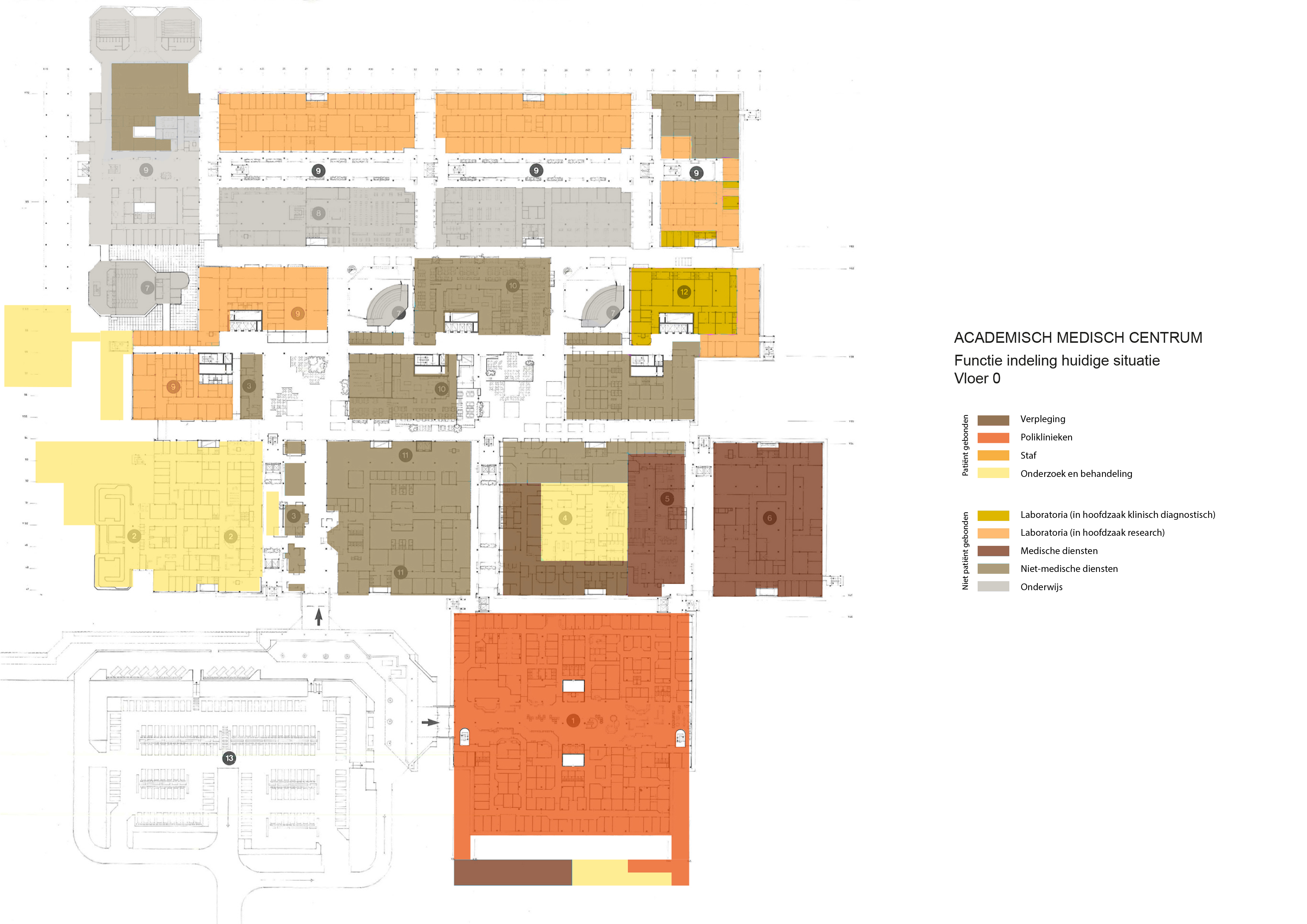



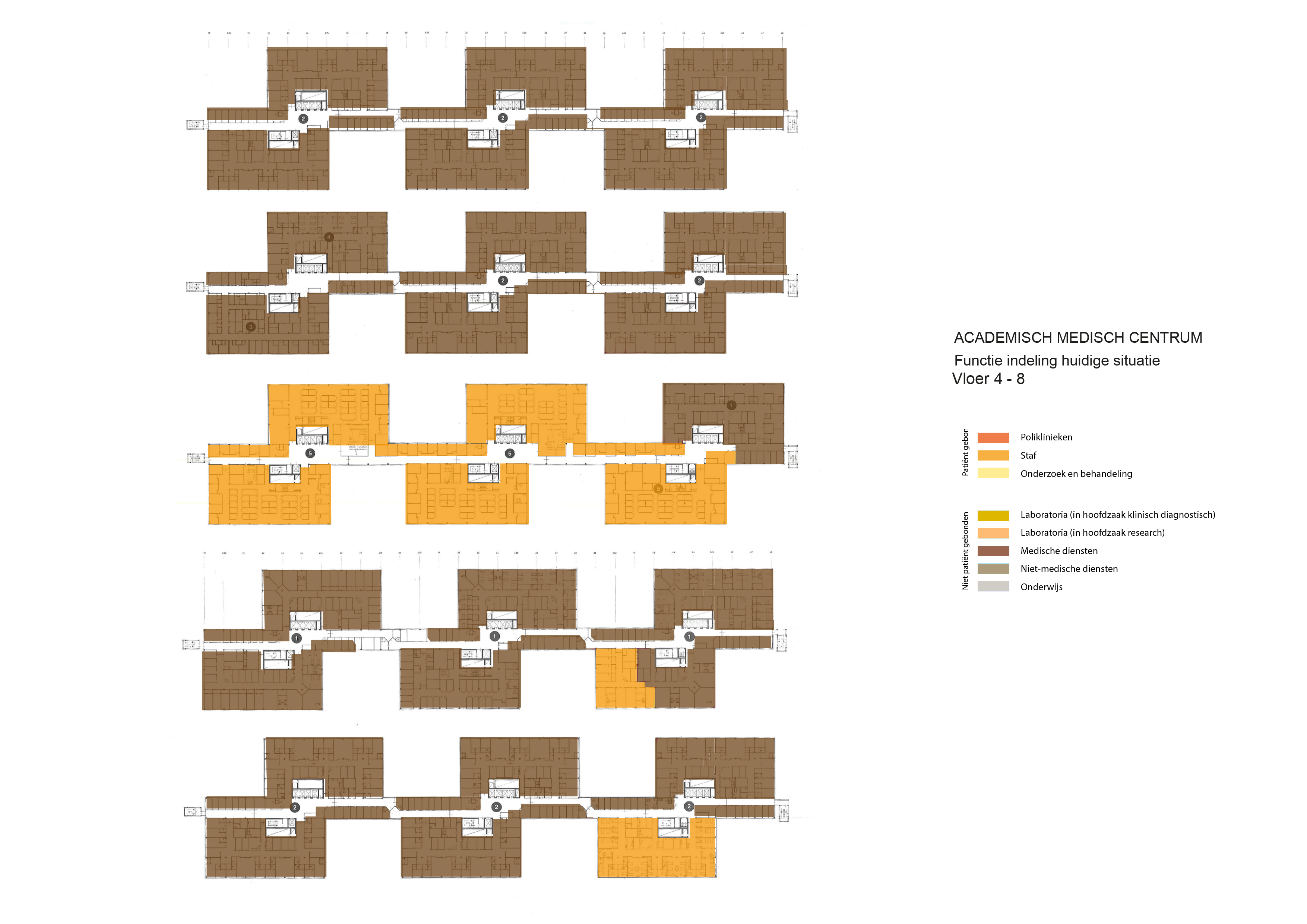
The floorplans of the AMC with function analysis.(AMC, 2016)
Specialism
The AMC has various top-referral specialties. These include cardiovascular diseases, immunology and infectious diseases, diseases of the digestive system (surgery and internal medicine), metabolic diseases, gynecological oncology, specialized care in early pregnancy, prenatal diagnostics, pediatric oncology, pediatric immunology/ hematology, vascular disorders of the brain, severe hearing disorders, schizophrenia, amyotrophic lateral sclerosis (ALS) and deep brain stimulation for severe obsessive-compulsive disorders. Besides these specialties the AMC has also been allocated various top clinical functions by the Dutch government. These are functions that provide medical treatments and services in limited number of hospitals, this due to high costs and required expertise. The AMC’s allocated top-clinical functions include kidney dialysis and kidney transplantation, open heart surgery, radiotherapy, neurosurgery, neonatology and nuclear medicine.
The AMC tries to distinguish itself from other hospitals through seven core areas of medical research. These are: cardiovascular diseases, immunity and infections, gastrointestinal diseases, metabolic disorders, neurological and psychiatric disorders, oncology and epidemiology & public health. All of these core areas covers the whole spectrum of medical research: from fundamental biomedical, translational and clinical research to the evaluation of new medical methods and techniques.
Infectious diseases and immunity
In a Dutch and international context, AMC researchers are working on the development of drugs and the evaluation of combination therapies for HIV/AIDS. Another line of research focuses on the development of vaccines, and bacterial research concentrates on pneumonia, meningitis and septicemia. Treatment options for rheumatoid arthritis are also being studied, with researchers concentrating mainly on the inhibition of proinflammatory proteins by means of an inactivated virus. Phagocytes, dendritic cells and T-cells are the central focus of fundamental immunological research.
Oncology
Most of the research in the core area of oncology concerns the molecular and biochemical backgrounds of cancer. There are four lines of research: gastrointestinal oncology, hematological oncology, pediatric oncology and neuro-oncology. The focus of the research is the hypothesis that only cells of one certain type – called cancer stem cells – cause tumors to grow and spread. The pediatric oncology research covers everything from fundamental research (genetic profiling) to clinical research. Much attention is focused on new drugs, and the later effects of oncology therapy.(AMC, 2009)
cardiovascular diseases
immunity and infections
gastrointestinal diseases
metabolic disorders
neurological and psychiatric disorders
oncology
epidemiology & public health
The seven core areas of medical research, own image.
AMC's development vision and aims
A hospital is in constant change, to guide this change the AMC has set up a vision and aims, this has also been the case for the redevelopment. Truthful to the original design principles the redevelopment vision for the AMC incorporates flexibility and standardization but also adds the new principles of safety and patient-centrality into its vision. Because of these last two principles the AMC aims to separated the different phases of care and than relocate them accordingly within the health care system. This in order to reduce errors and increase patient centrality. These phases include diagnostics, treatment, screening, after care, nursing and caring. In order to suite patients within the hospitals patient care units redevelopment is mandatory since the current ones have sunk under an acceptable level for modern medicine. While solving that problem another problem of patient care unit vacancy can be tackled.
While one of the AMC's aim is to place a larger focus on patient centrality the hospital currently struggles to do show with its current design. One of the aims therefor is to adjust and change the wayfinding, approach and entering of the hospital area and the hospital. The current main entrance and the polyclinic entrance are out dated, not representative and don't contribute to the welcome feelings patients and visitor should have. It is the AMC that envisions these problematic aspects solved into an embracing routing in- and towards the building.
Important to the hospital is larger growing presence within the world of academical research, in quantity (promotions and publications) as well as quality (research funds and impact scores). It is important for the AMC to remain as one of the top UMC research institutes. Through international cooperation it remains a key player within its core areas as previously mentioned. To increase its international presence valorisation is promoted from start-up companies.
The research and treatment center forms the core of the AMC, these function feature high investment costs, complex housing and growth. The functions feature polyclinics, research centers e.g. but in the future the polyclinic functions need to grow. In order to achieve this sub functions have to be segregated, that would mean that research functions are supposed to be clustered as for the other functions.
Flexibility plays a role within the strategy to make more efficient use of the current facilities. This means that employees will have to share their office facilities with employees from other facilities. Therefore reducing 70 offices spots per 100 employees. Another aim is the redevelopment of internal spaces so that they can be used for one main purpose like offices, waiting, research, consultant rooms e.g. and not just for one specific department.(AMC, 2016)
Redevelopment constraints
The board of the AMC has made the decision to not demolish the building complex. That brings with it that transformation and renovation is a considerable option for them. But with these come restrictions, demands that the AMC has set up in order to maintain an certain appearance and values embedded within the architecture. But transformation and renovation brings difficulties with it, for one is that a hospital is not simply able to shut down for a long period of time while construction takes place. Appointments, surgeries and treatments are scheduled far ahead. While at the same time various functions require sterile facilities. Sterile research samples cannot easily be transported without external factors influencing the sample. In short the transformation of a hospital is very difficult. Luckily the large city like building provides the opportunity to temporary shut down one of their various fragments. The constraints that are set by the AMC are:
1. During transformation the hospital should remain in function. That would imply that a phased development plan should be developed.
2. The redevelopment should remain within the current boundaries of the building. Excluding the entrances of the building and the renewed landscape plan.
3. The concrete structure should remain in place and should remain visible.
While the first and second constraints are very clear and logical to implement in the new design. I believe the third one to more debatable. While the AMC wants to keep not just the interior but also the exterior concrete structure visible. In my opinion a transformation within the architecture of the AMC should result into an new architectural intervention. Therefor part of the concrete structure including the facade should be transformed into the new architectural intervention.
1. Remain active while construction
2. Building boundries
3. Concrete structure
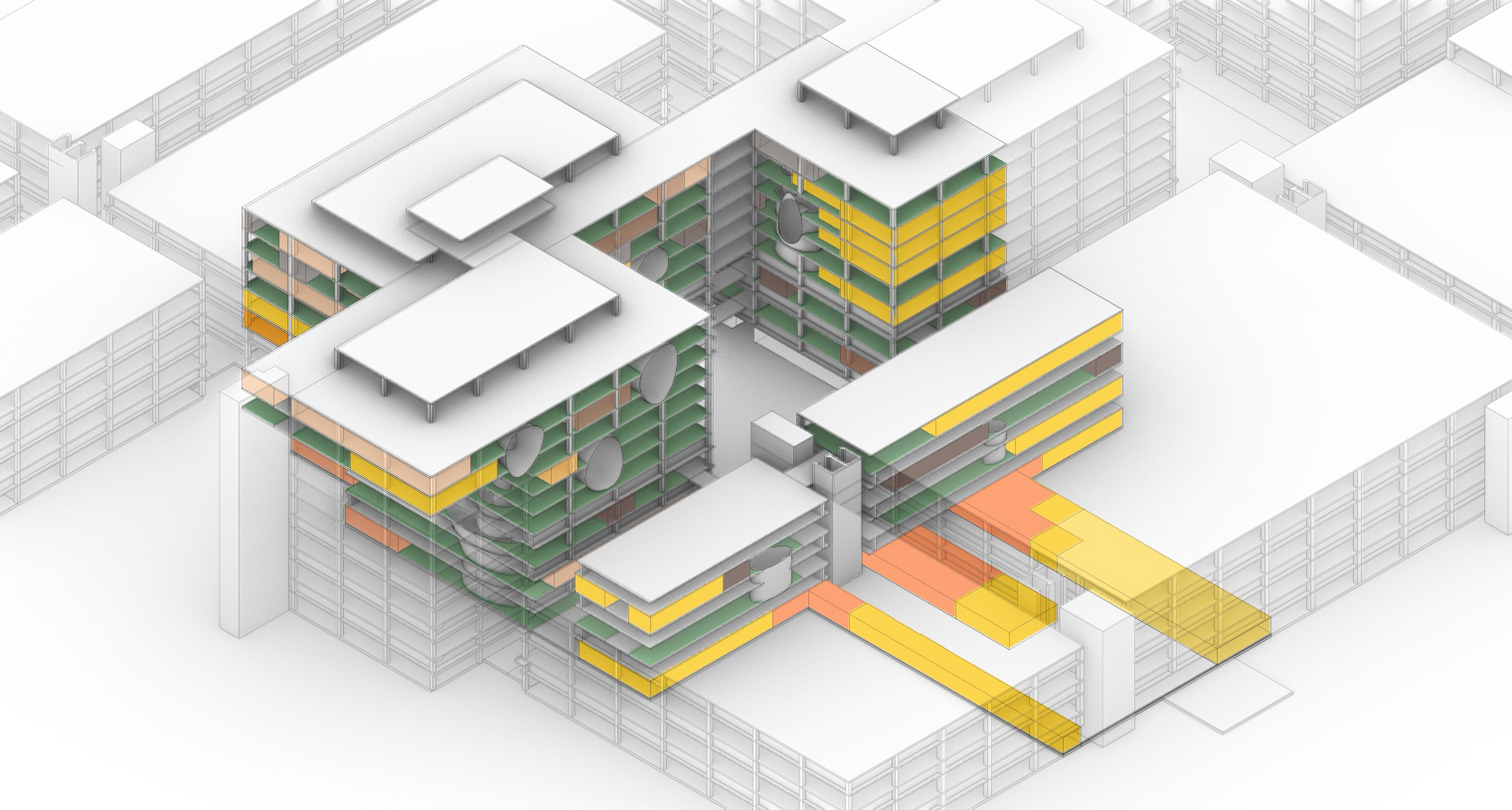
The Design Void
Medical centers are complicated buildings to design, often these buildings house a wide range of different functions with each of them having different requirements. In order to house these functions hospitals tend to be very large. This can clearly be seen when someone looks at the Academic Medical Center. Therefor a (re)design of a hospital building is very time consuming. Unfortunately this assignment is being done within the graduation track and there the time that is required for this redesign is not available within the graduation course. Therefor the design will be focused on a specific fragment.
It is this fragment that I will redesign into a state of the art hospital design. Incorporating the previously mentioned restrictions, aims and visions set by the AMC.
The design fragment of the academic medical center.
The functions
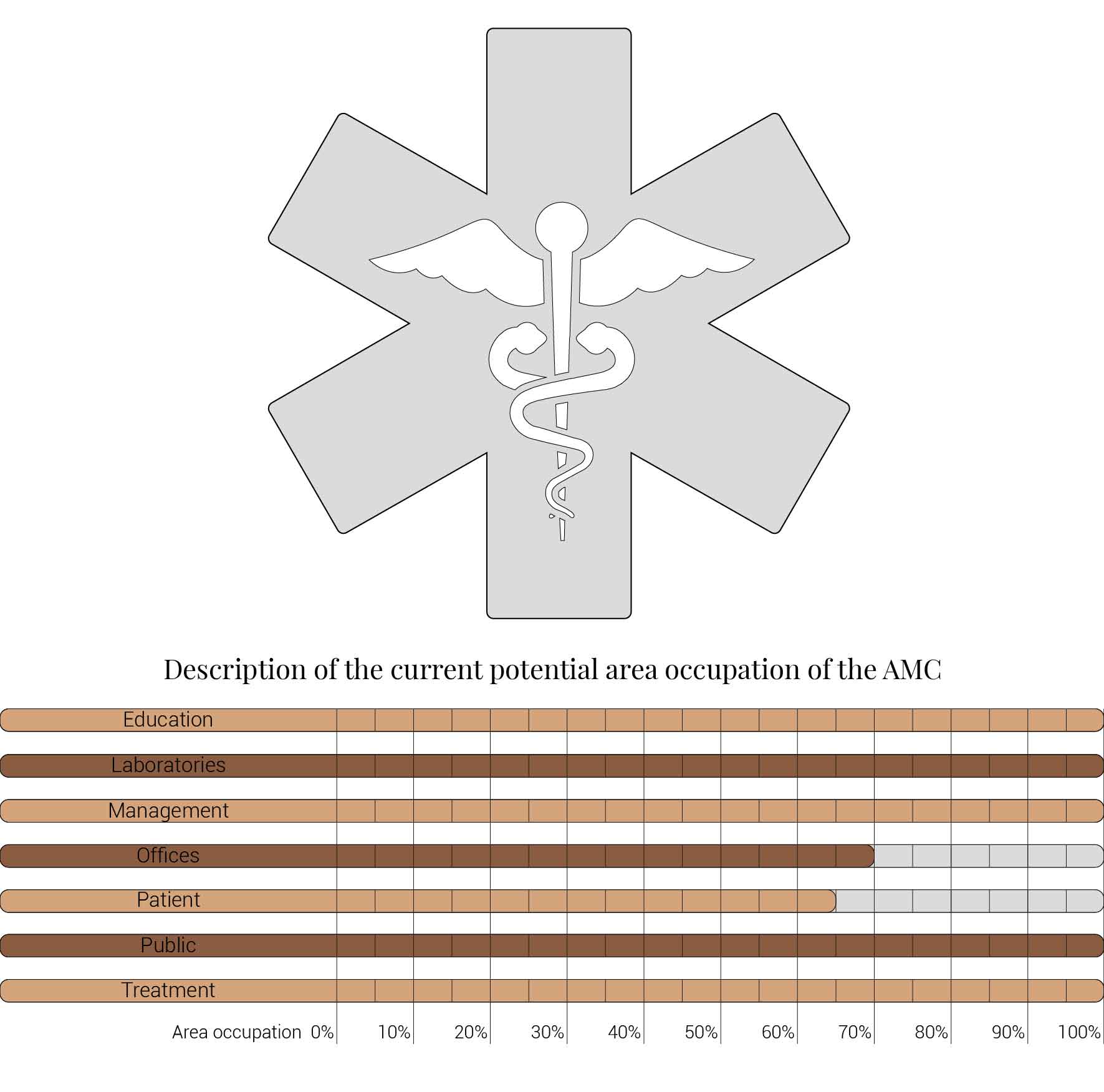
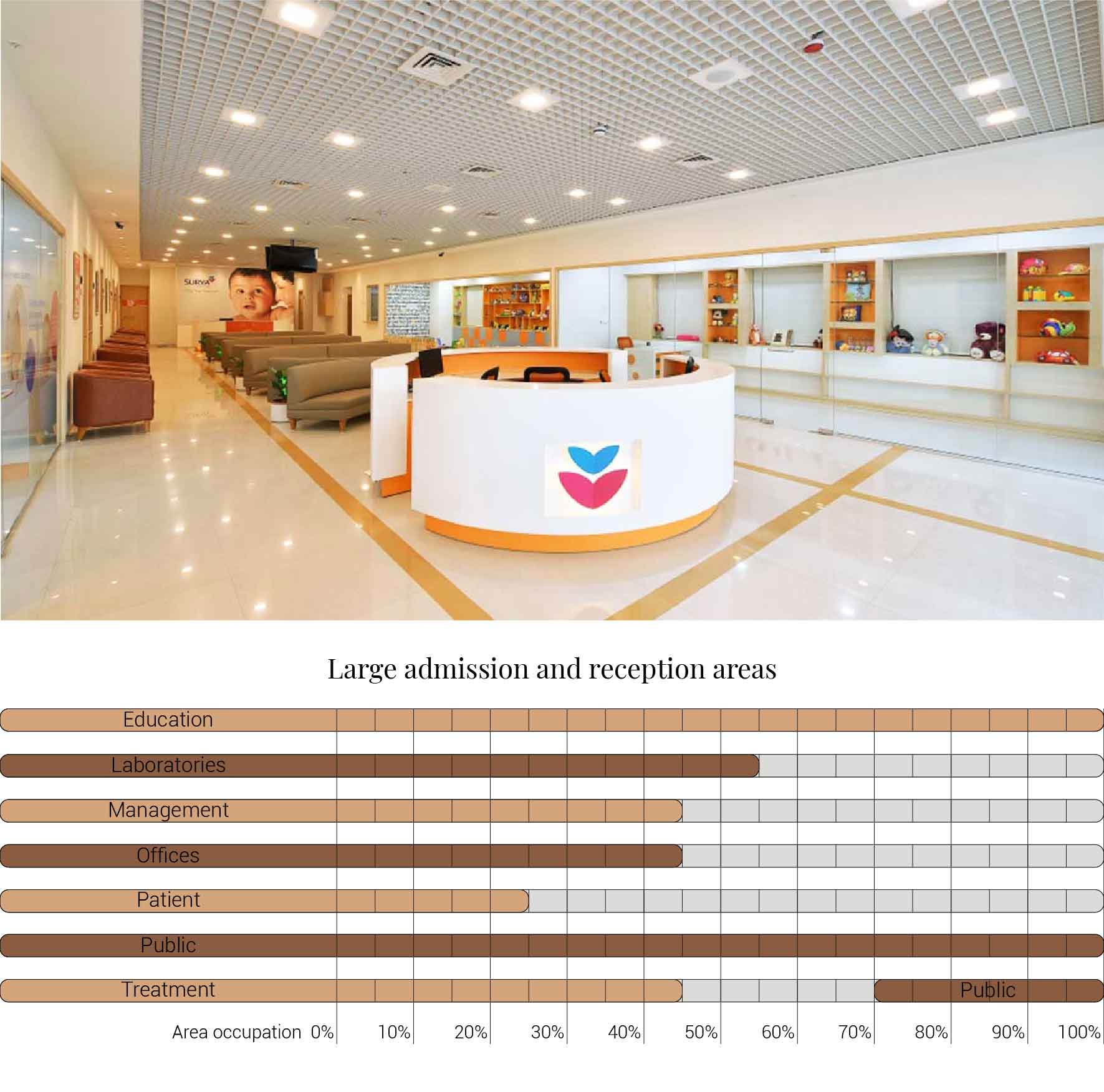
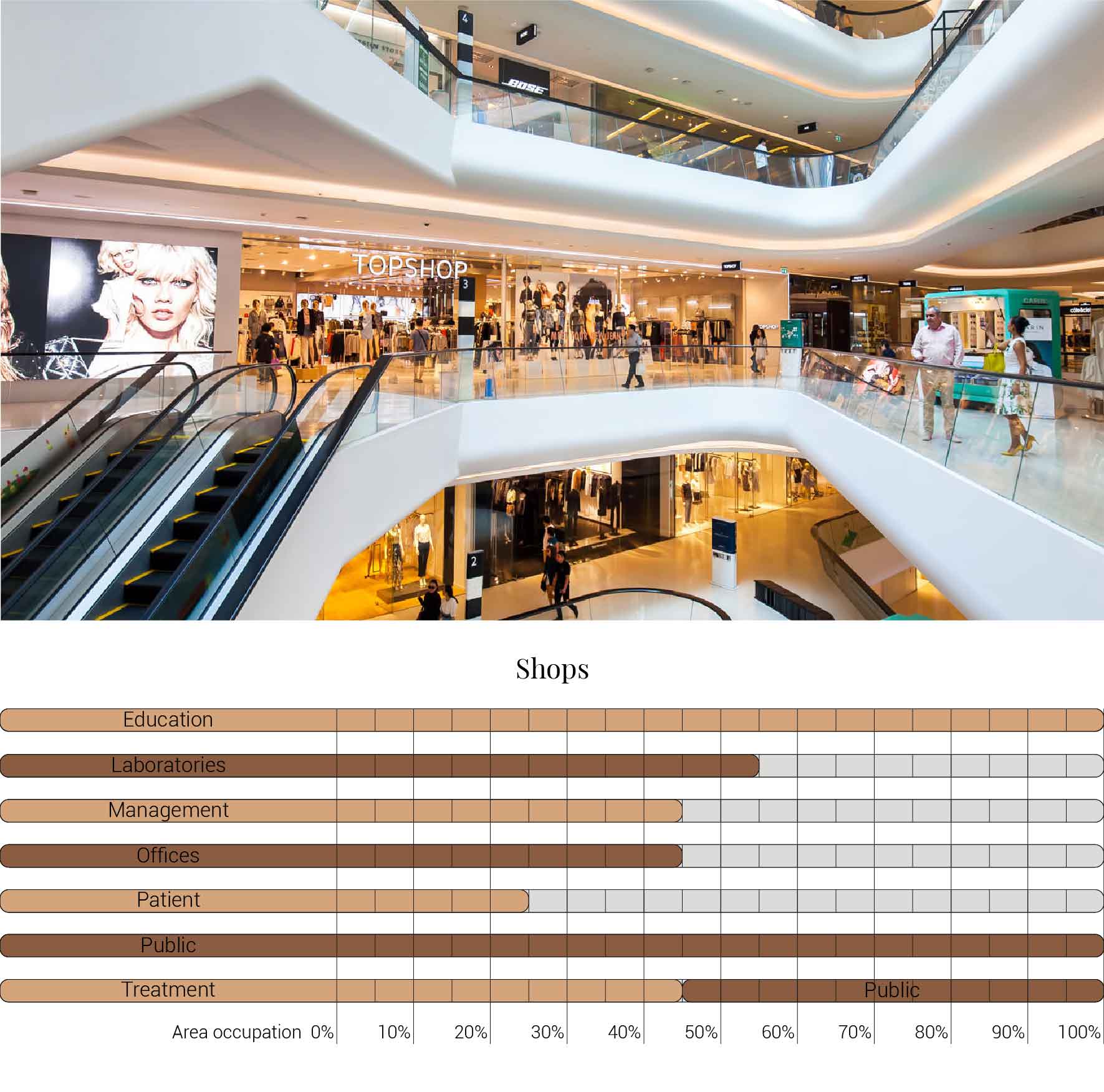
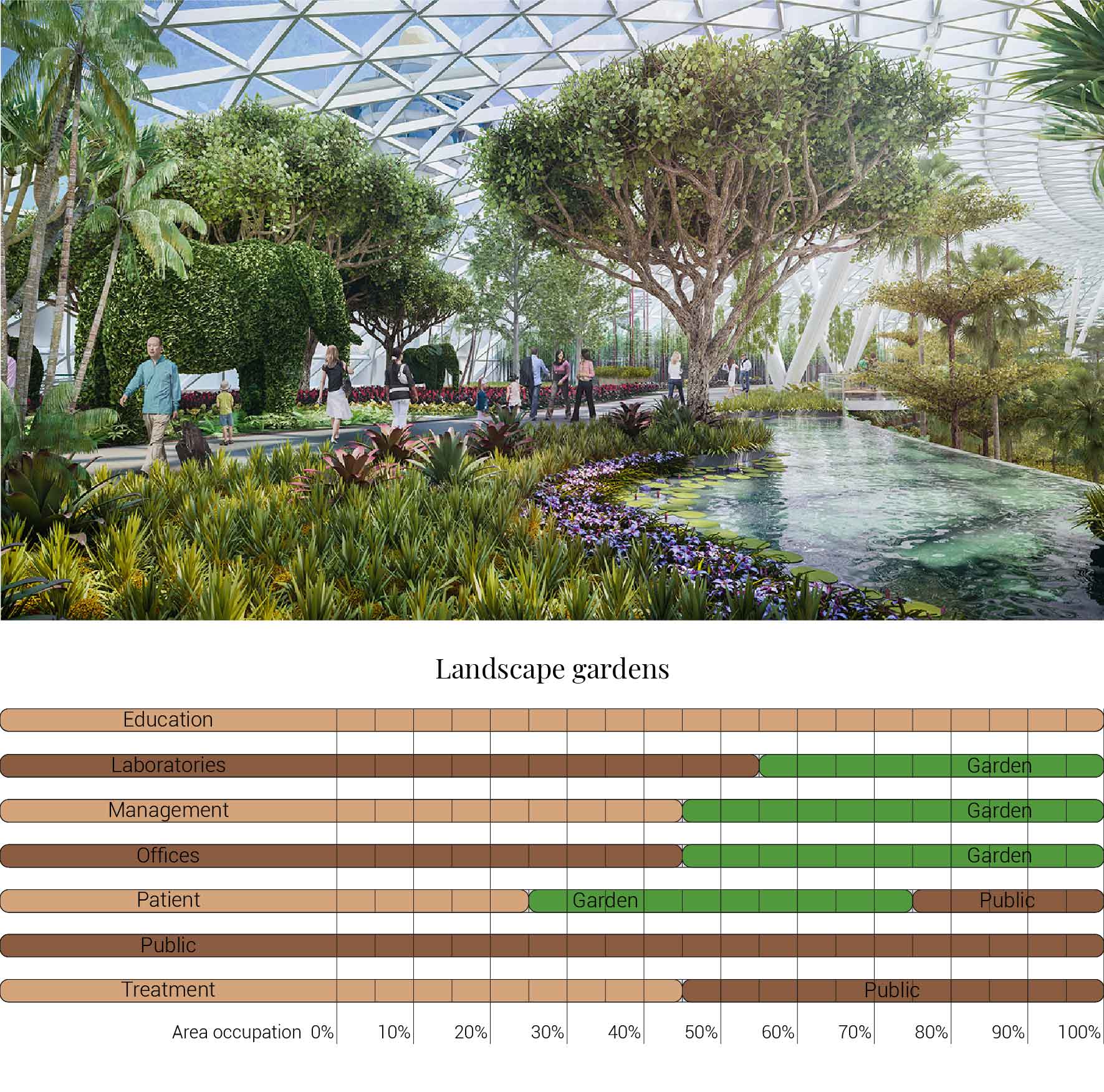
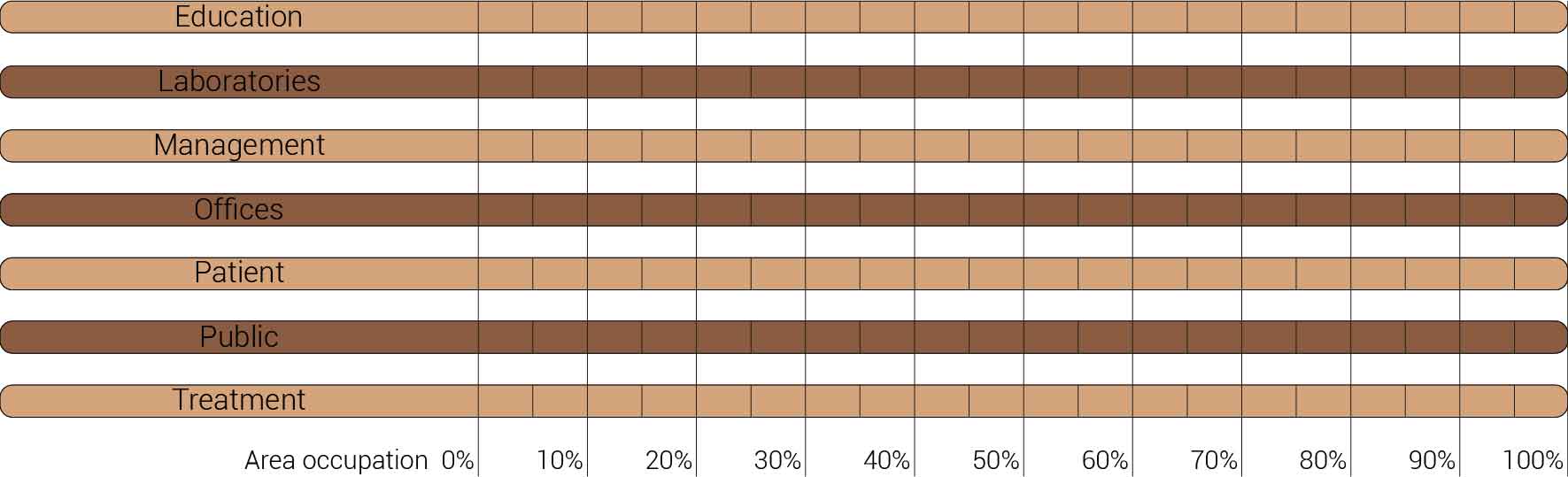
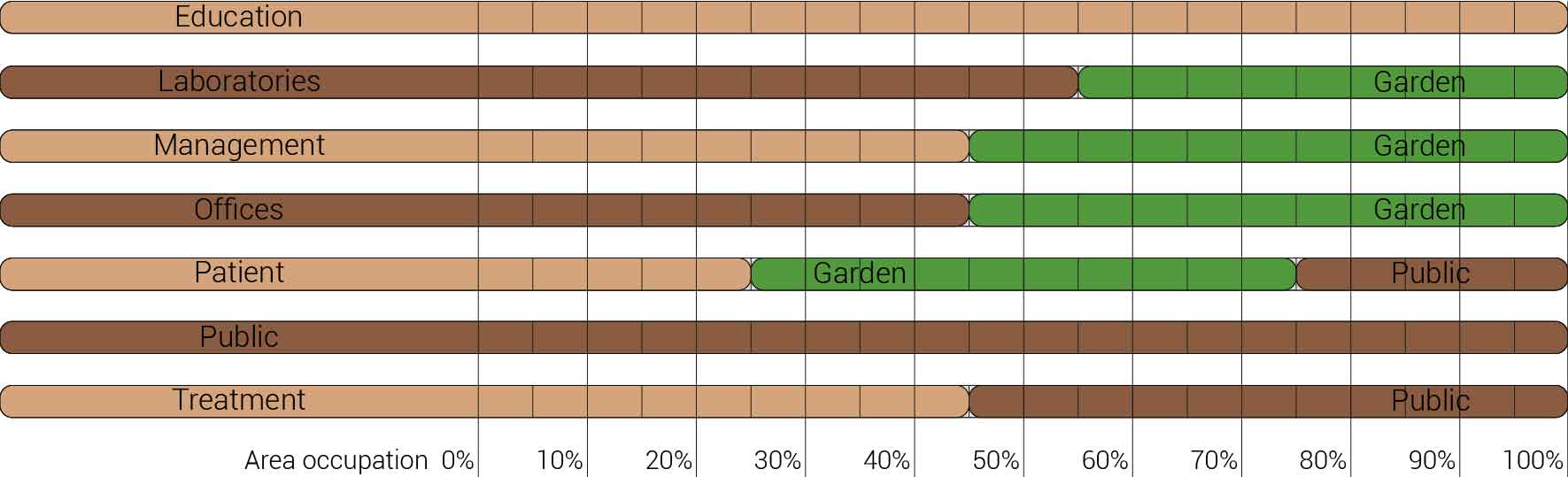
The decision to transform just a fragment of the building implies that I also had to reduces the amount of functions that I am able to incorporate into the design. The original fragment is home to varies functions which I have to decided to once again use as input for the new. The functions that originally are housed in this segment are, the main entrance, lecture arena, lecture rooms, toilets, varies laboratories and treatment facilities with their own specialism, shops, restaurants, offices, patient care units, nurseries and many more. But the basically can be reduced to the functions as shown below. What this image also shows is that these functions and areas are used as relative for comparing the area occupation of the building to the new situation.
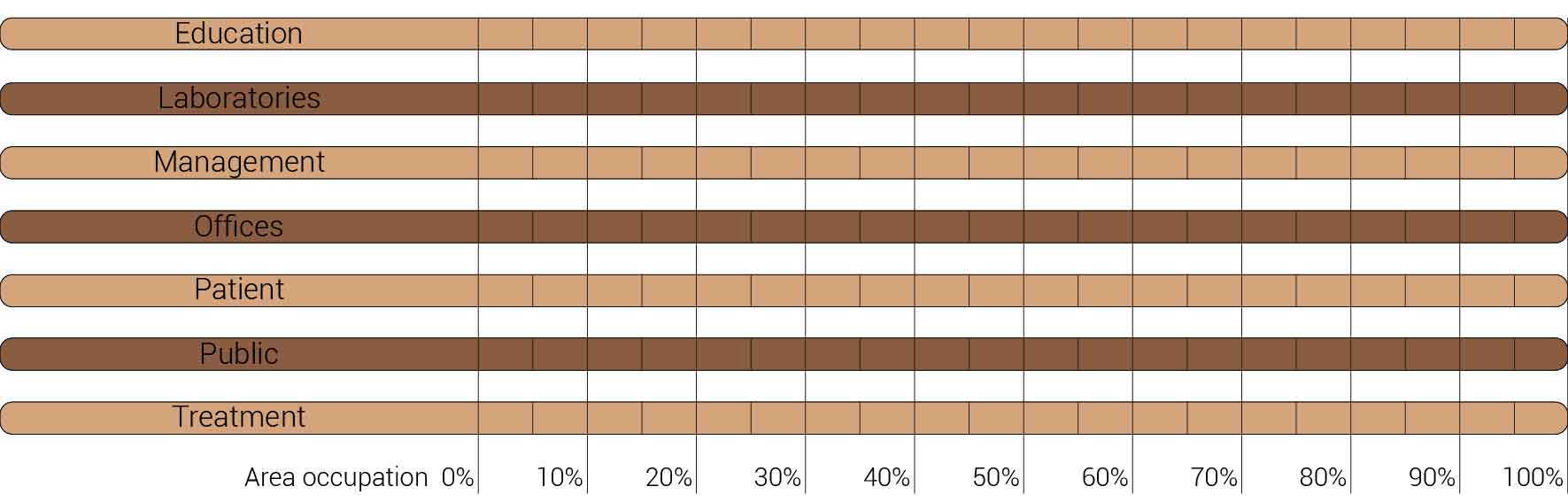
Overview functions and their occupation.
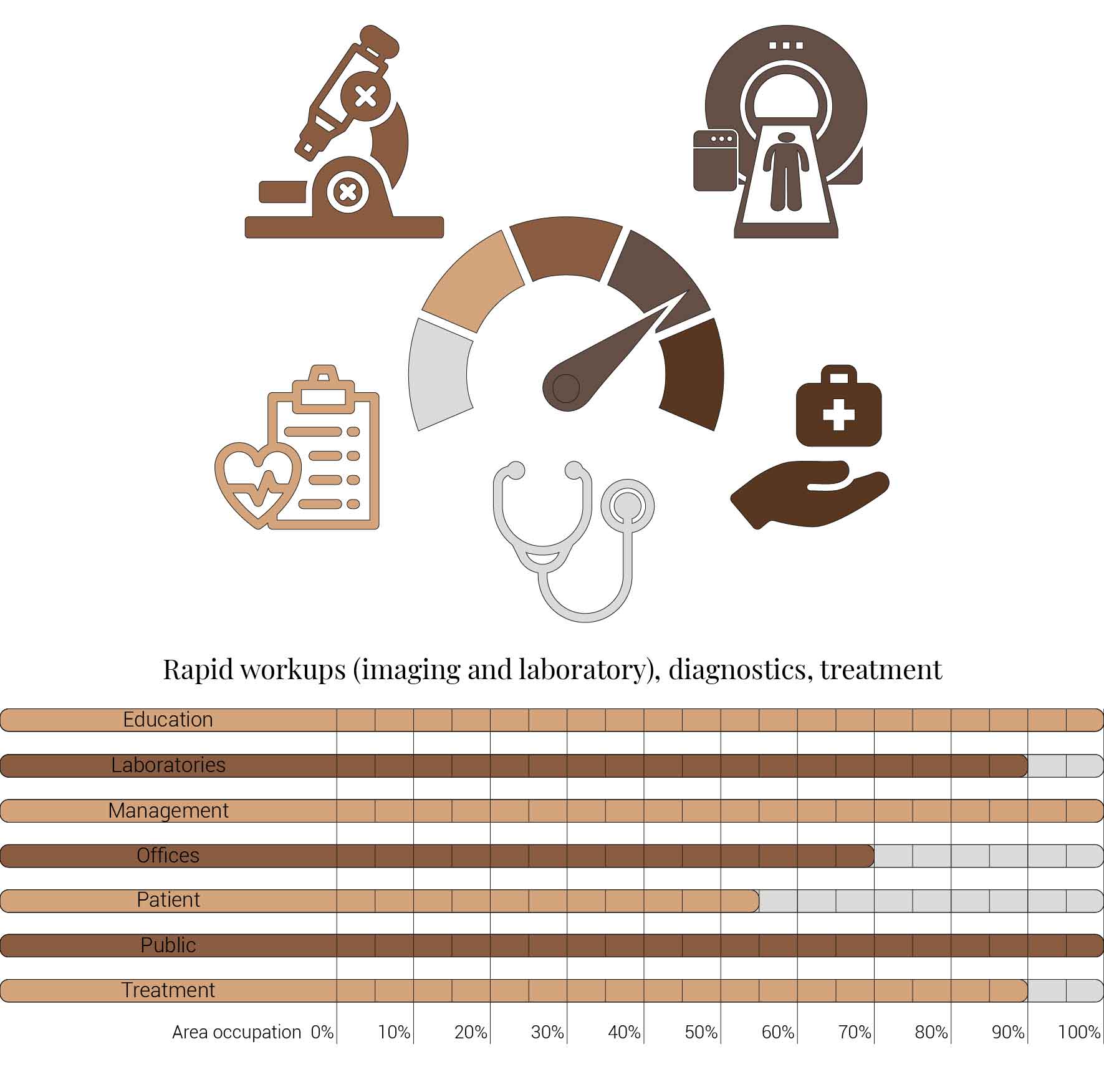
Within the section about the AMC's vision and aims it already had been stated that currently the AMC is struggling with hidden patient care unit vacancy. As a result of this vacancy one out of the three pcu towers could be repurposed. Since my fragment houses one tower the area occupation can already be reduced to sixty six percent. But it does not stop there the AMC aims to reduce the amount offices currently in used from hundred office places for hundred employees to seventy offices places per hundred employees. Therefor also leading to a reduction of thirty percent resulting in the area occupation as shown below. This area occupation will form the basis for the further space reductions.
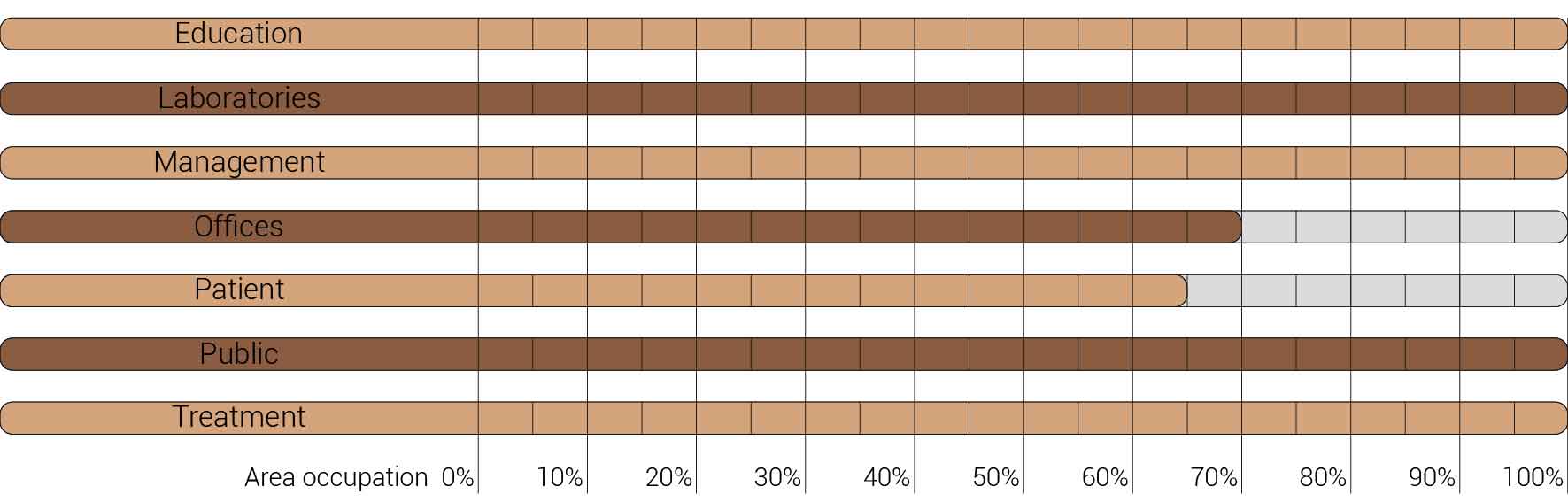
Overview functions and their occupation, renewed.
The future of healthcare and the hospital
Survivability is at the core of every human being. Everything we do we do to survive and prolong our existence as humankind. In order to live longer and survive diseases we have developed a large and complex healthcare system. One shackle within this system is the hospital. This place is designed as a last resort, a last chance for the ill to get better. Since the hospital is a place for healing and becoming well, it would imply that being within a hospital would be experienced as a pleasant experience. But on the contrary people often experience anxiety and discomfort.
This is due to that same survivability, it is when we become ill we become uncertain. We lose the control of the situation of health. As a consequence of this uncertainty it becomes difficult to predict what will happen next. Which then can result in feelings like isolation, alienation and depression. These feelings do not improve the potential for regeneration. Patients can suffer from increased blood pressure, stress, reduced sleep.
But this is not what a hospital should cause any patients. It is here where architecture could play a role, a role to prevent these negative emotions from ever occuring and put patients at ease. Research done to find out which design factors matter to patients to create a healing environment. It proposes six themes with associated design characteristics to improve the healing environment; Spatial comfort, Privacy, Autonomy, Sensory comfort, Safety and security, and Social comfort.
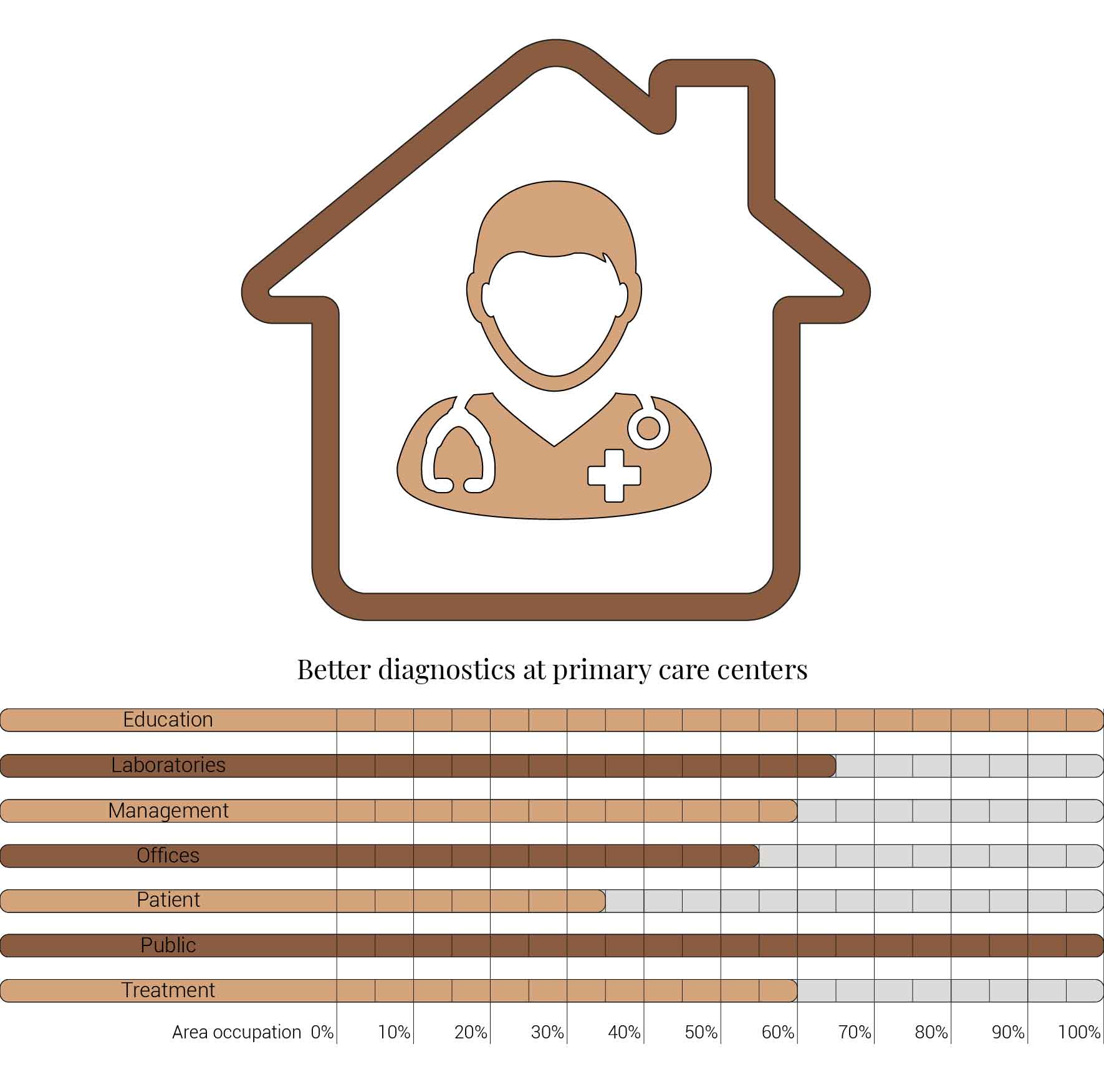
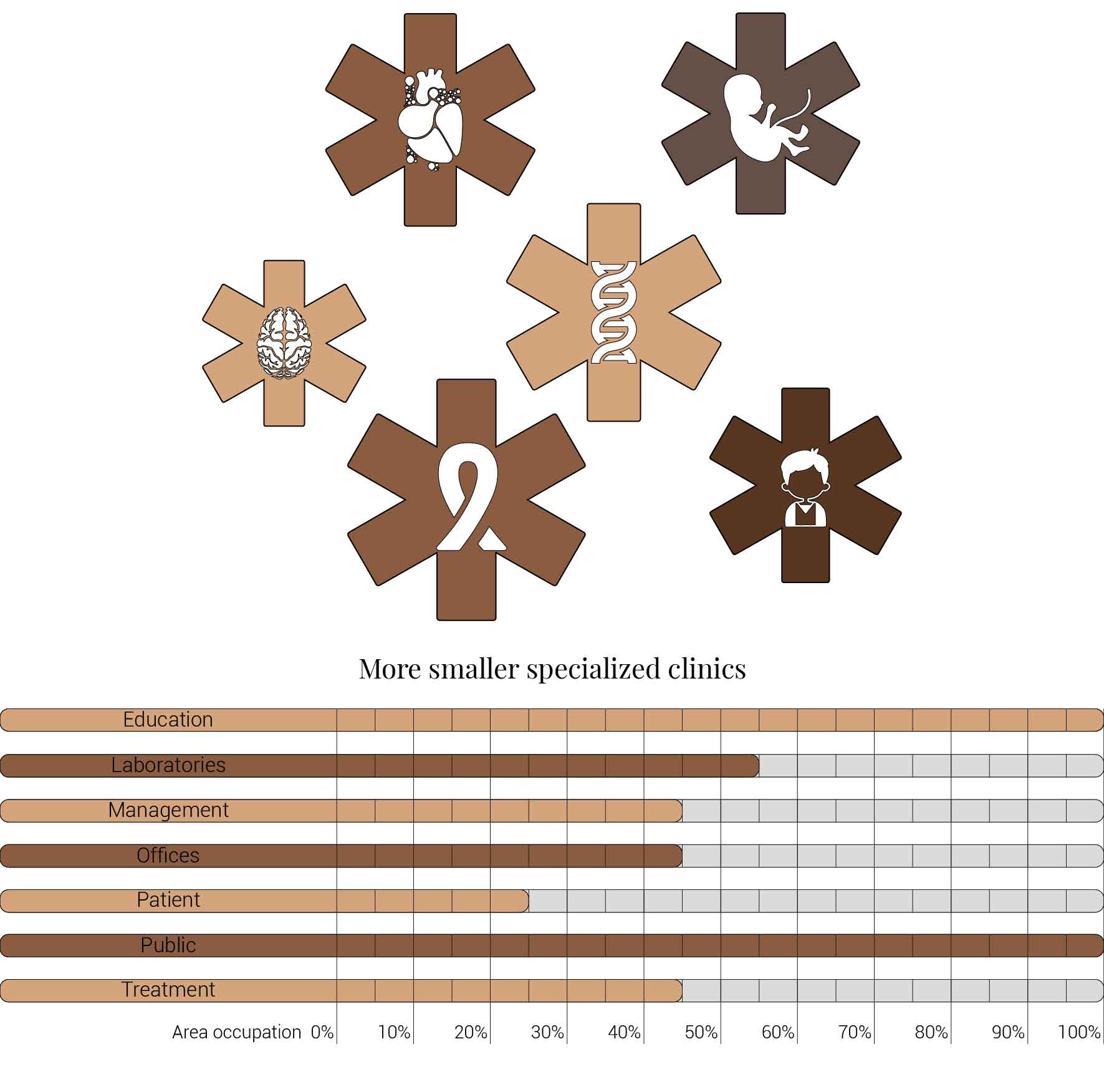
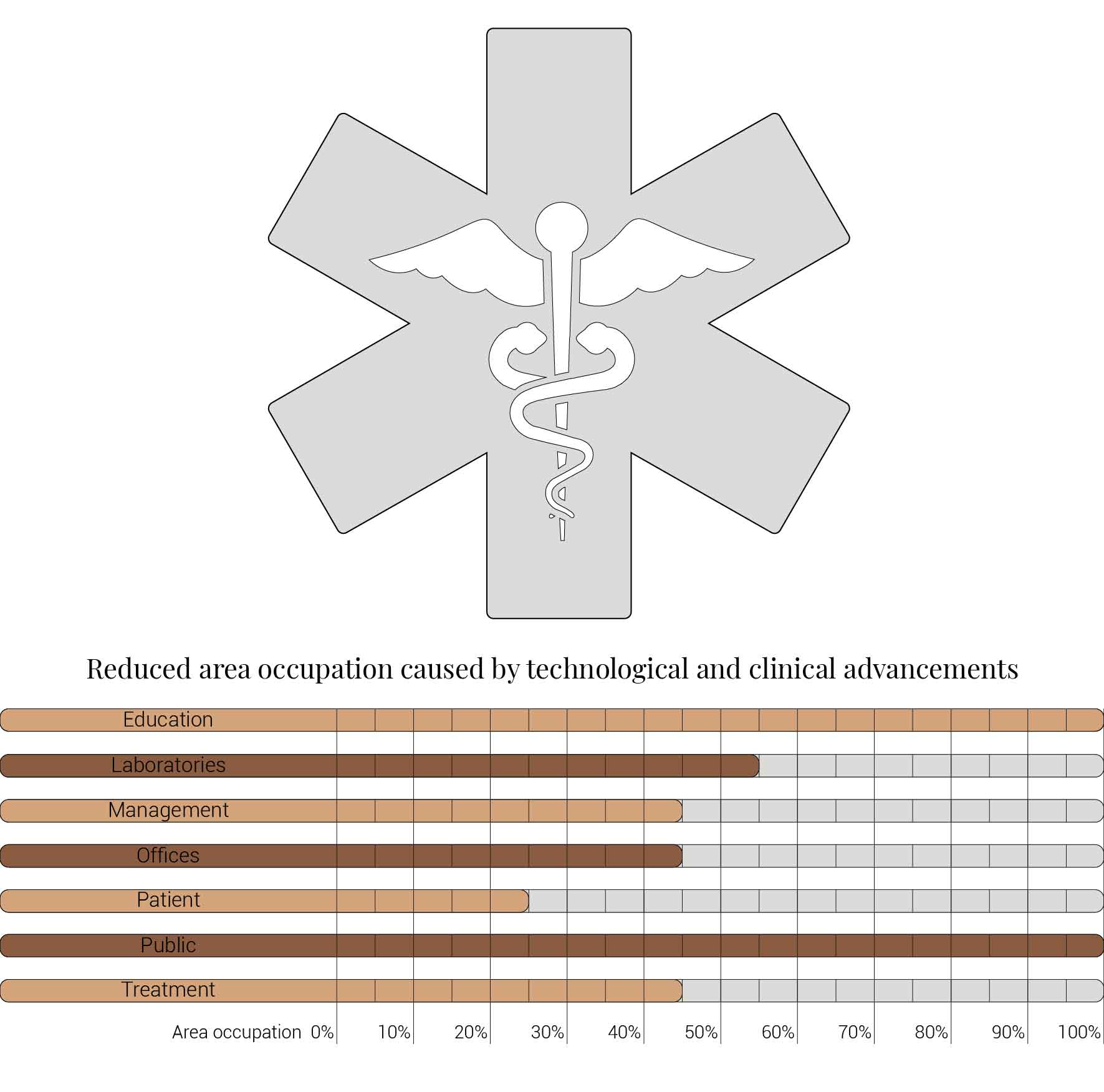
Hospitals will be smaller
On of the future prospects for hospitals is that they will shrink in size. This reduction is cause by various different influences. These influences are often caused by technological and clinical advancements with influences on different functions within the hospitals. For the design of the fragment these advancements have different impacts on the different spaces.
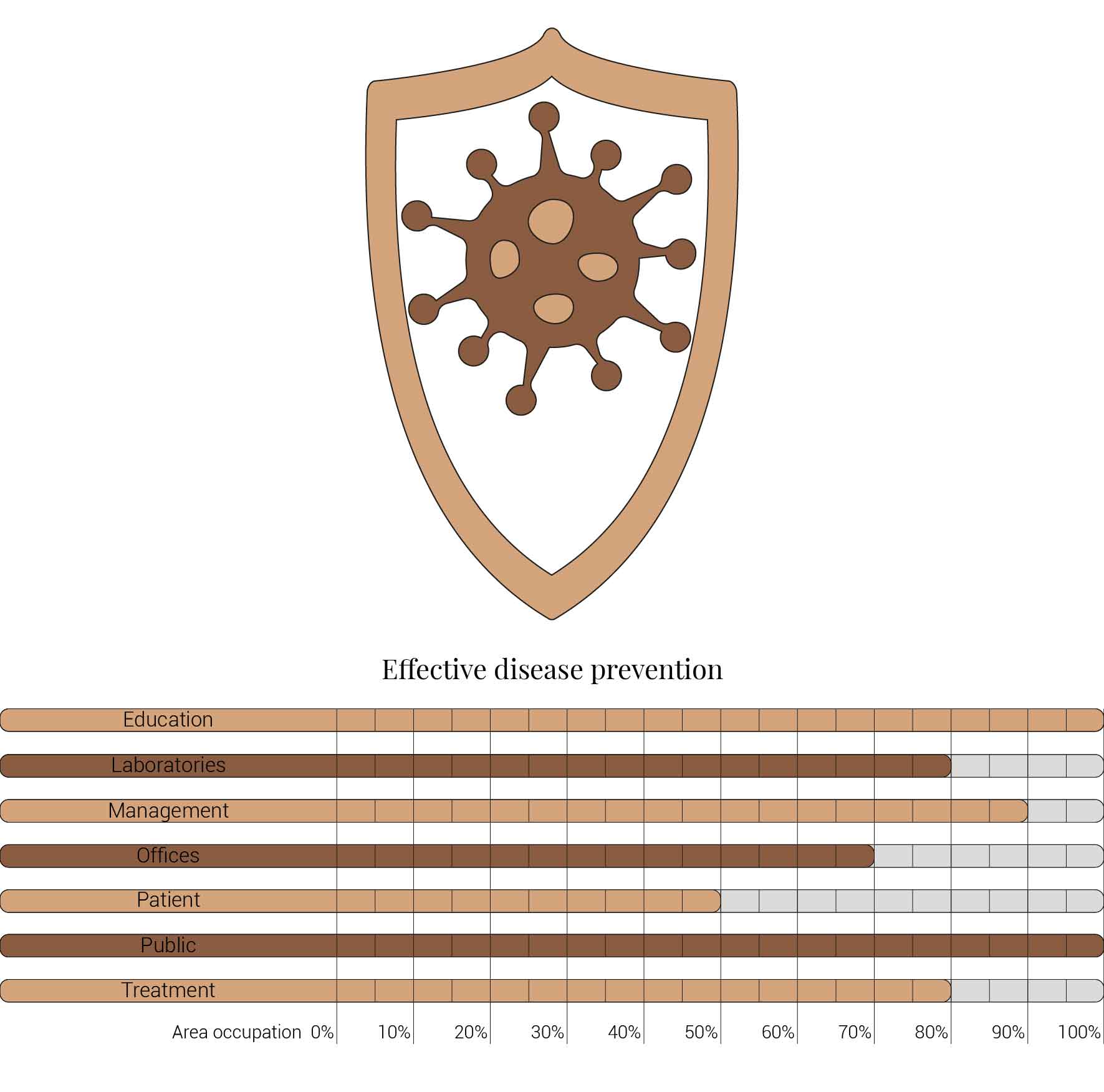
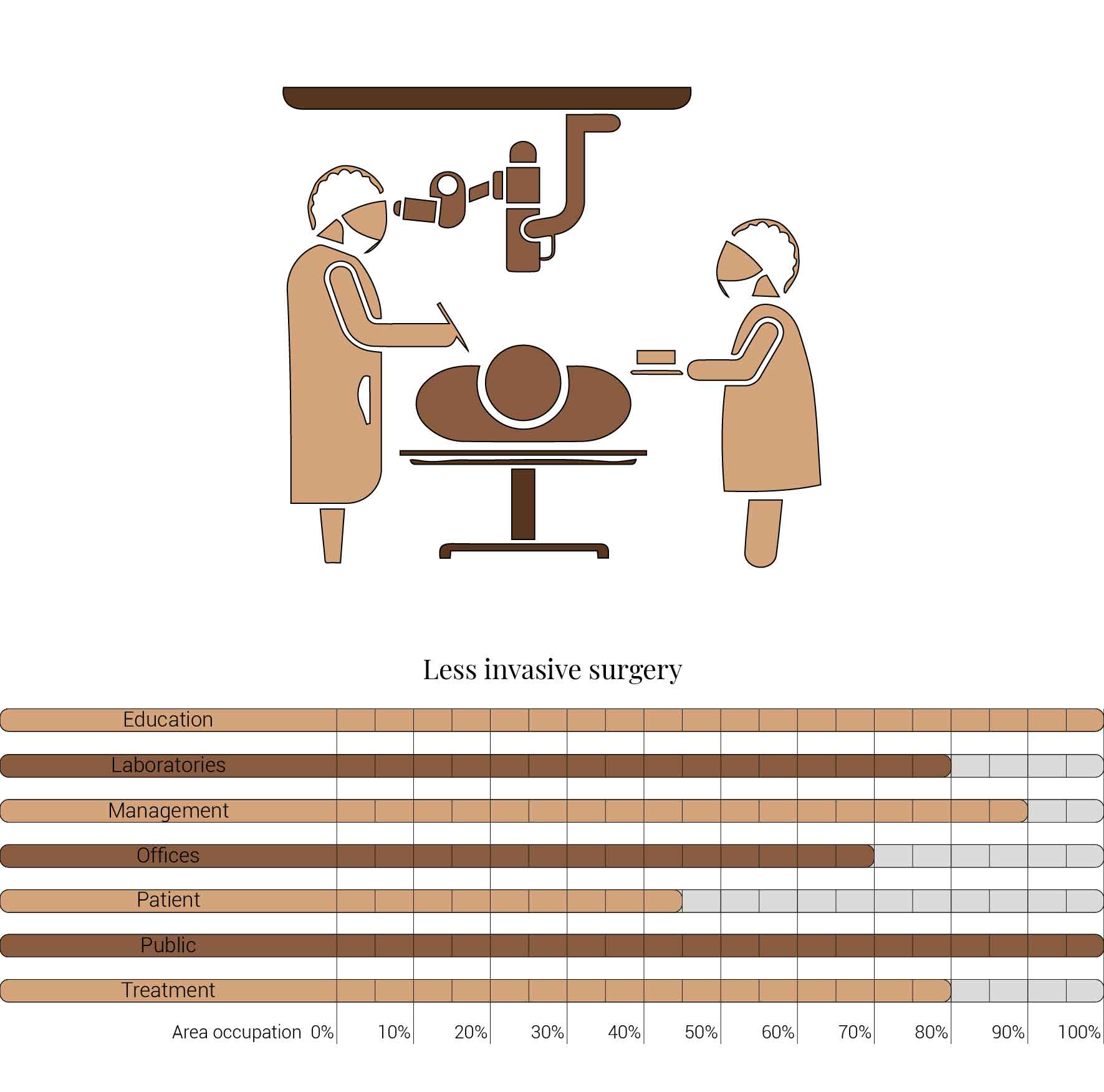
Build up of the various variations.
The user friendly hospital
As mentioned in the introduction, hospitals are often experienced as user unfriendly, as impersonal healing machines. That aspect will change in the future. The balance is slowly shifting towards an hospital which centralizes the patients. Reducing the negative impacts of on health while simultaneously improving the aspects of regeneration. That shift also impacts the architecture of the hospital increasing the needs for extra functions. The impact for the AMC is shown below.


The various aspects of a user friendly hospital.
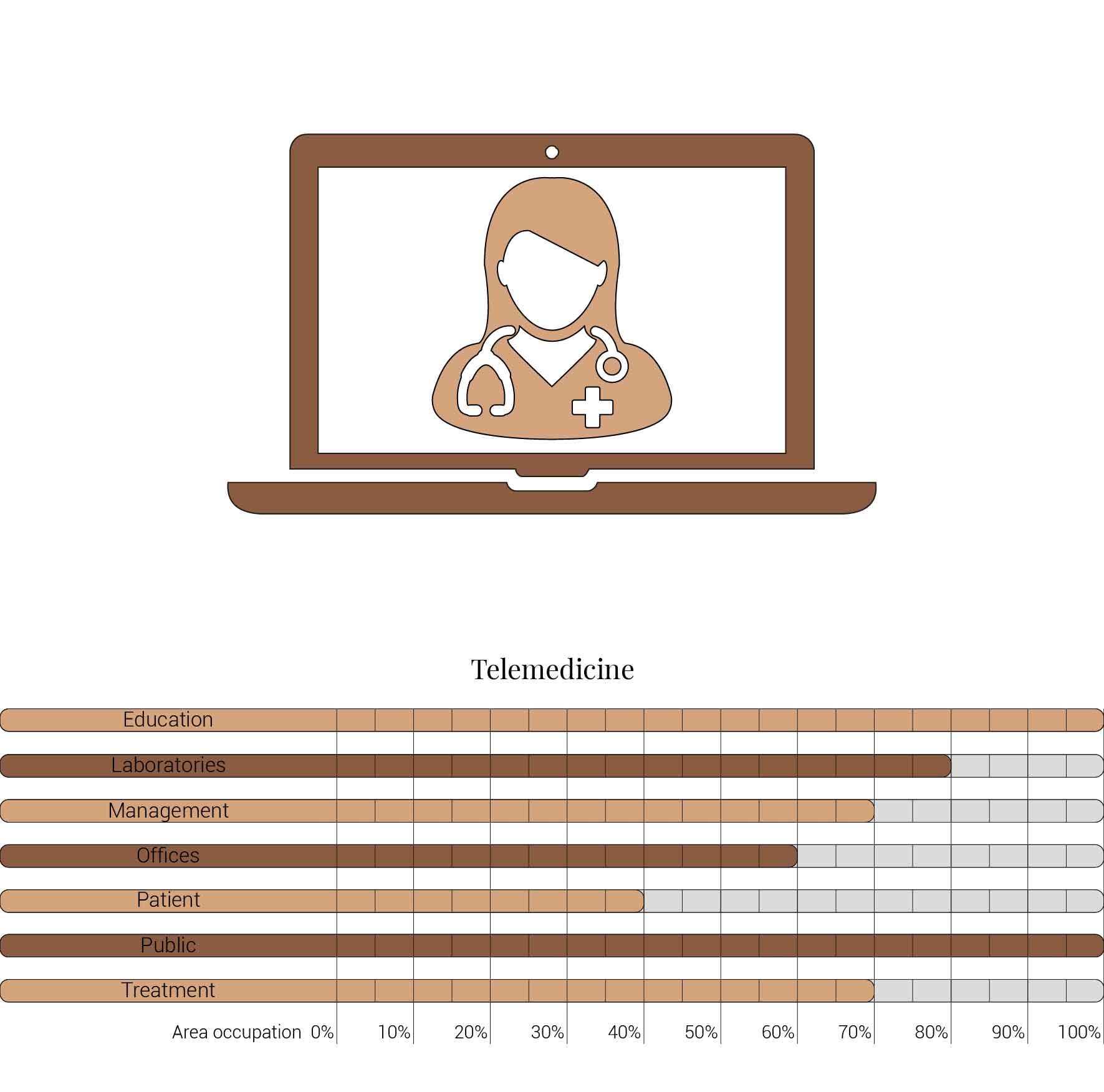
Telemedicine will be everywhere
Electronic medical records in connected health, primary care, demografic, diagnosis, lab, medicarion, medical history, digital health data, big data, Surgery through machinery.
Personal health records (PHRs)
Patient portals
Mobile health and medical apps
Communication tools and social networks
Wearable technologies and sensors
Robots will be more present and visible
New technologies and research fields
molucalar, nano, genome, personalised medicine, Virtual and augmented reality, 3d printed organs.
The patient, health and healthcare
But this is not what a hospital should cause any patients. It is here where architecture could play a role, a role to prevent these negative emotions from ever occuring and put patients at ease. Research done to find out which design factors matter to patients to create a healing environment. It proposes six themes with associated design characteristics to improve the healing environment; Spatial comfort, Privacy, Autonomy, Sensory comfort, Safety and security, and Social comfort.
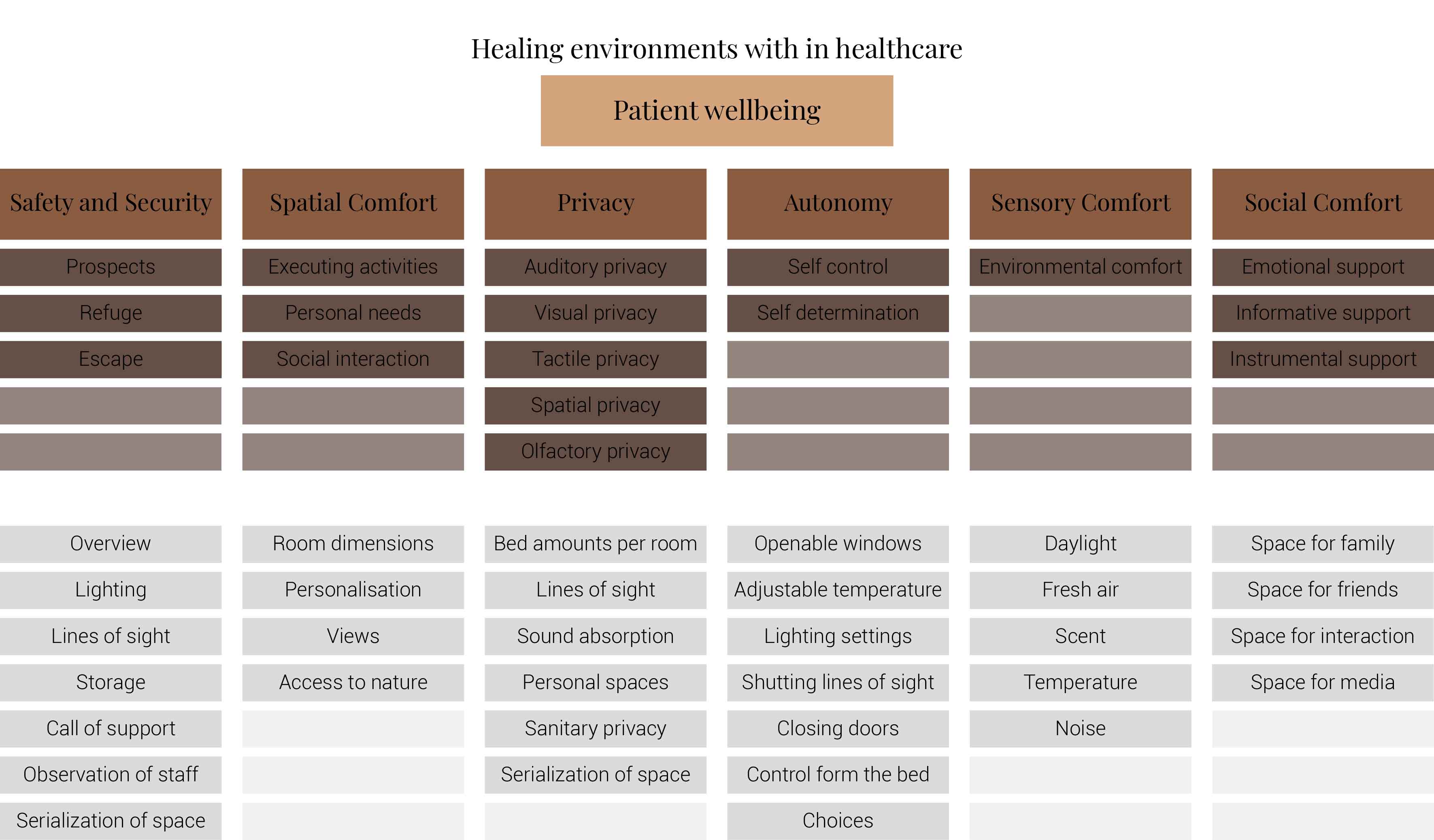
A summary of design characteristics based on the six themes
This image is based on (Schreuder, Lebesque, & Bottenheft, 2016)
The purpose of the research was to find out which design characteristics are more important to the patients than others. Concluding with an advice on which factors should be paid with more attention. It has founded that if hospitals would be transformed into healing environments they should focus on the spatial comfort, safety and security, autonomy and their associated design characteristics.
For spatial comfort it would mean that rooms should be large. It should provide views with sky and green, appealing materials, personal storage space, and space for private conversations.
When it comes to safety and security within the hospital patients appreciate a clear transition form public to private, where unauthorized persons will have restricted access to certain areas. Within the rooms focus should be on lighting, safe personal storage and the ability to call personnel from the rooms.
Many of these characteristics already show some form of autonomy. Another important factor is for patients to have their own influence on what food and drinks the patients consume.But also the possibility to determine resting periods, indoor climate settings and inclusion with decision for treatment.(Schreuder, Lebesque, & Bottenheft, 2016)
While designing all the six themes matter and all their corresponding design characteristics but these previously mentioned characteristics should be integrated with larger importance.
The Design
The functional distribution
Based on the future predictions the area occupation of the AMC will change radically in comparison to what it is now. Therefor the AMC requires a new functional distribution. It is in this new functional distribution where the patient can once again be centered within the architecture design process. In order to achieve this I have created an grasshopper script which tries to reduce the distances between related functions (see the figure below). These relations are shown in the adjacency matrix below. In the beginning this script does not yet use the reduced occupation but instead uses the current occupation. These functions and their area requirements are distributed on an projected grid. The Galapagos evolutionary solver component then shuffles all these functions on the grid, creating thousands of iterations, each having an different adjacency value. The lower the value the closer the functions should be located therefor patient walk distance is reduced.
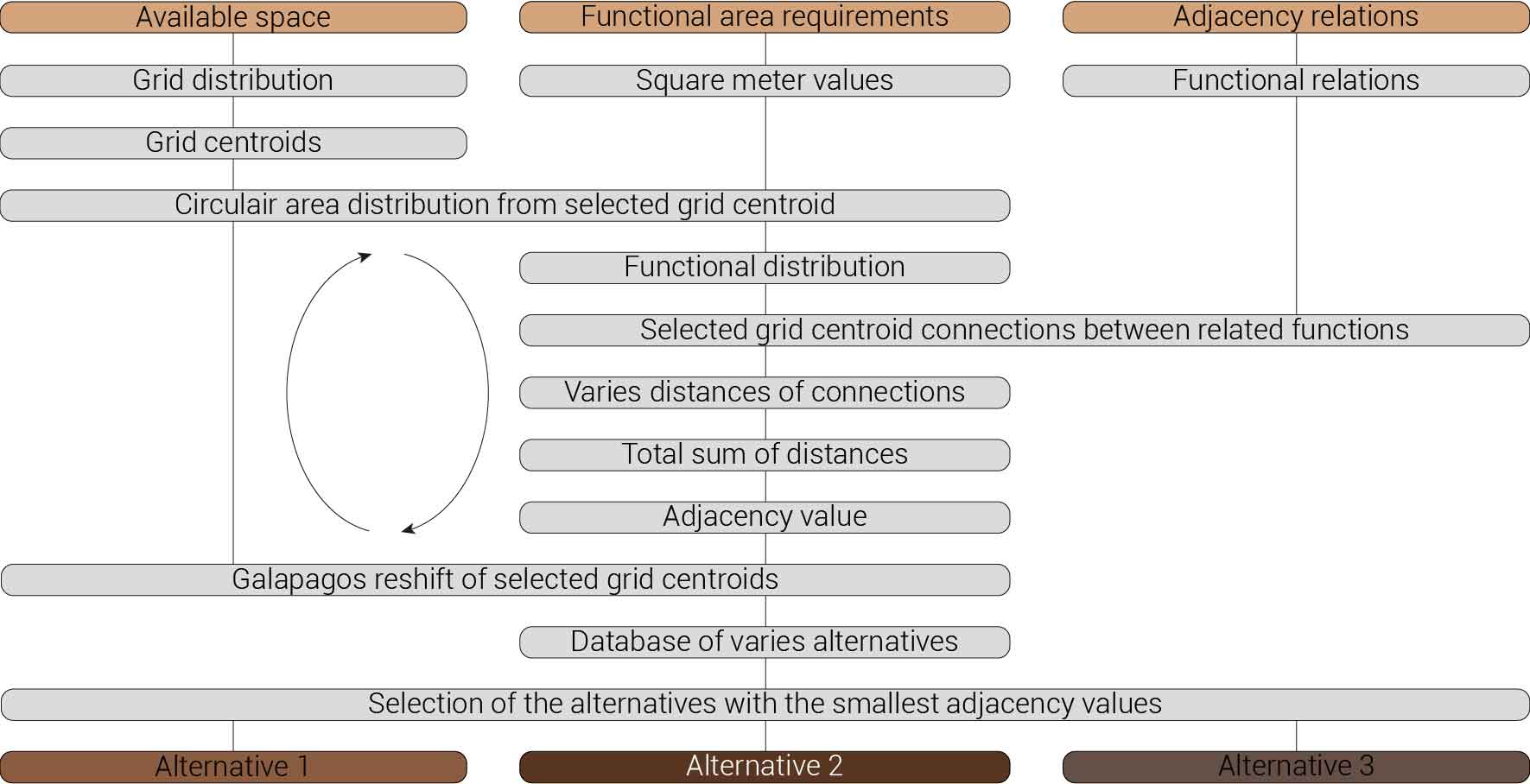
Computational design for the functional distribution.
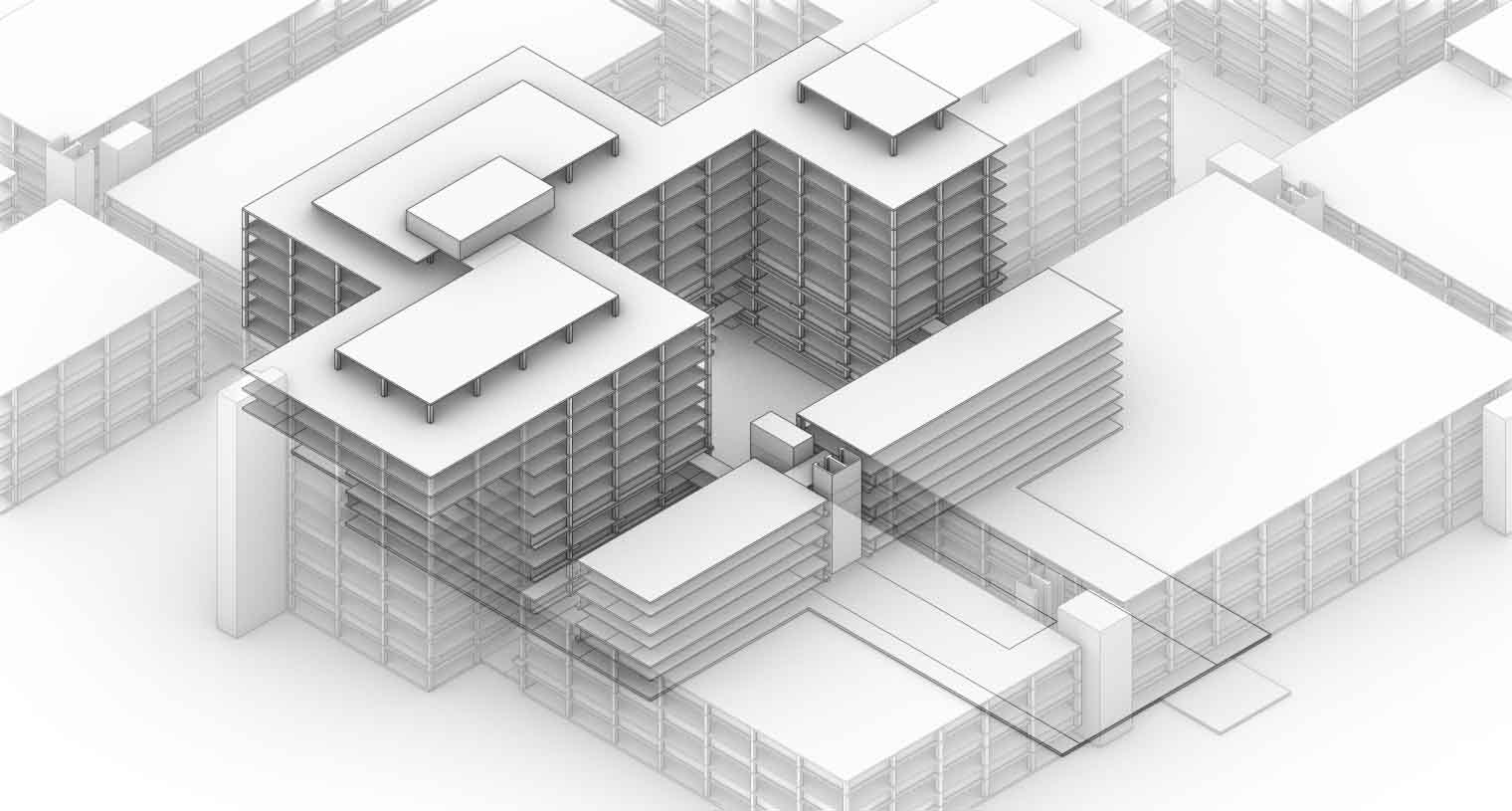
The design fragment for the functional distribution.
Overview functions and their occupation.
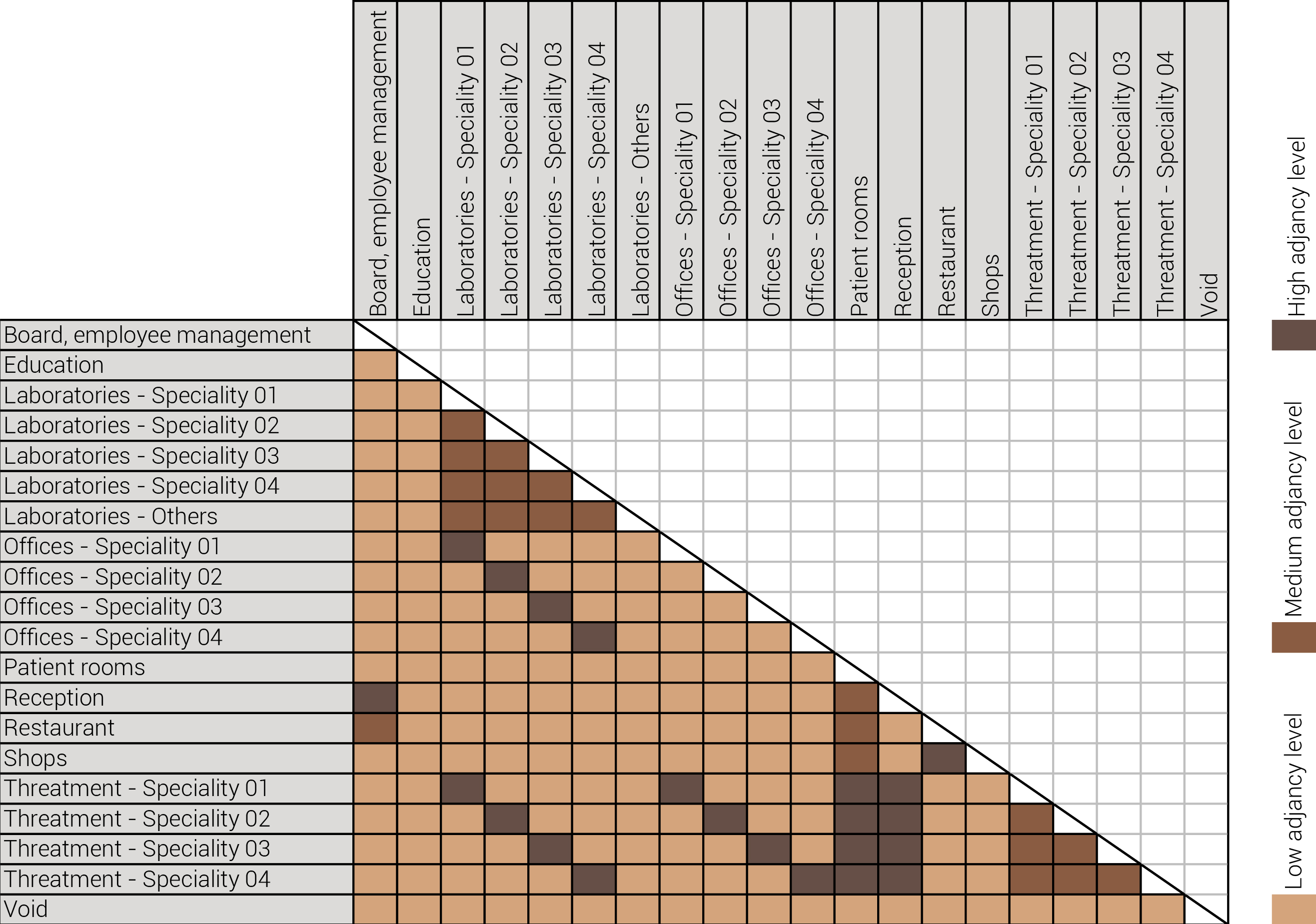
The adjacency matrix portraying the spatial relationship between the functions .
Various design solutions based on the adjacency matrix.
Based on the future predictions the area occupation of the AMC will change radically in comparison to what it is now. Therefor the AMC requires a new functional distribution. It is in this new functional distribution where the patient can once again be centered within the architecture design process. In order to achieve this I have created an grasshopper script which tries to reduce the distances between related functions (see the figure below). These relations are shown in the adjacency matrix below. In the beginning this script does not yet use the reduced occupation but instead uses the current occupation. These functions and their area requirements are distributed on an projected grid. The Galapagos evolutionary solver component then shuffles all these functions on the grid, creating thousands of iterations, each having an different adjacency value. The lower the value the closer the functions should be located therefor patient walk distance is reduced.
Build up of the top three variations.
The functional reduction
The next step from the functional distribution is to reduce the functions as it was argued before. That result being shown below once again. To arrive at this reduction four patterns are developed each decreasing the area occupation in its own way. These are; pattern one, from the centroid towards the outside. The second one, randomly reducing the area occupation. The third, from the outside inwards towards the centroid. And the last and fourth one reducing the the area occupation from the middle and expands its reduction towards the outside and inside. It is shown below what the impact of these patterns is one the space occupation on each floor. It than is up to me as designer to find the suitable configuration of patterns for each function. Hereby I took into account the impact these patterns have on creating connected open spaces. For this configuration I have used the design alternative with the best adjacency score, which is the first option.
Various design solutions based on the adjacency matrix.
Build up of the various variations.
Various design solutions based on the adjacency matrix.
The vertical connection

The design fragment for the functional distribution.
The functional distribution

The design fragment for the functional distribution.
The functional distribution

The design fragment for the functional distribution.
Various design solutions based on the adjacency matrix.
Various design solutions based on the adjacency matrix.
Fungi
Introduction
This project revolves around the growing of architecture by application of mycelium. Mycelium is the vegetative part of fungi. This biological tissue/ material is composed from tube-like fibers. These fibers are called hypha and are approximately 1 lm in diameter. Hypha grow by elogation of the apical tip. Which means that the fibers grow faster in the tips than in its branches. On occasion these fibers branch out and merge with other hyphae. As a consequence a random fibernetwork structure is formed; The mycelium (Lull et al., 2005).
The hyphae network
Mycelium can be grown in multiple forms, (pure) mycelium, synthetic mycelium and composite mycelium. The last one will be the main focus of this material study since this is the form that is most used within the product development and the built environment. The composite is a mixture of mycelium mixed with a organic substrate most preferably a lignocellulosic biomass. Mycelium than forms it's network of hyphae on and through the substrate by (partly) consuming the substrate. It then transforms the substrates biomass into chitine (up to 45%), Protein and polysacharides. As a result of this process mycelium and the substrate are bonded into the mycelium composite (Tazelaar, 2017).
Mycelium composite
Pure mycelium
Synthetic mycelium
Structural properties
The usage of mycelium as a building component is relatively new. Therefor there is not much research available involving this subject. Besides that mycelium is a biocomposite with many different possibilities for substrate, that fact makes it even more harder to determine average structural properties. In the table below structural properties are shown of mycelium in comparrision to EPS and concrete. EPS is shown since the characteristics of mycelium and EPS are very similiar as are their usages within product development. While concrete is shown as it is a widely used within the build environment.
As seen the structural properties are very similair when it comes down to their compressive strengths. While the young's modulus shows that mycelium is more flexible than EPS. With the mycelium flexibility it is also able to better deal with flexural forces than EPS. But the best the reason why mycelium is better for usages than EPS is its low energy consumption for production and it's biodegradable properties.
| Mycelium Composite | EPS | Concrete (C53/65) | |
|---|---|---|---|
| Density [Kg/m3] | 122 | 20 | 2500 |
| Compressive strength 10% [MPa] | 0,12 | 0,10 | 65 |
| Tensile strength [MPa] | - | 0,15 | 2,13 |
| Flexural strength [MPa] | 0,23 | 0,15 | 4,30 |
| Young's modulus [MPa] | 1,14 | 6,00 | 37300 |
This table is based on information from (Cement&BetonCentrum, n.d.;Tazelaar, 2017)
Acoustics
Fungi based composites show great potential in the usages of sound obsorption. As seen below its absorption properties are depending on the composite material used.
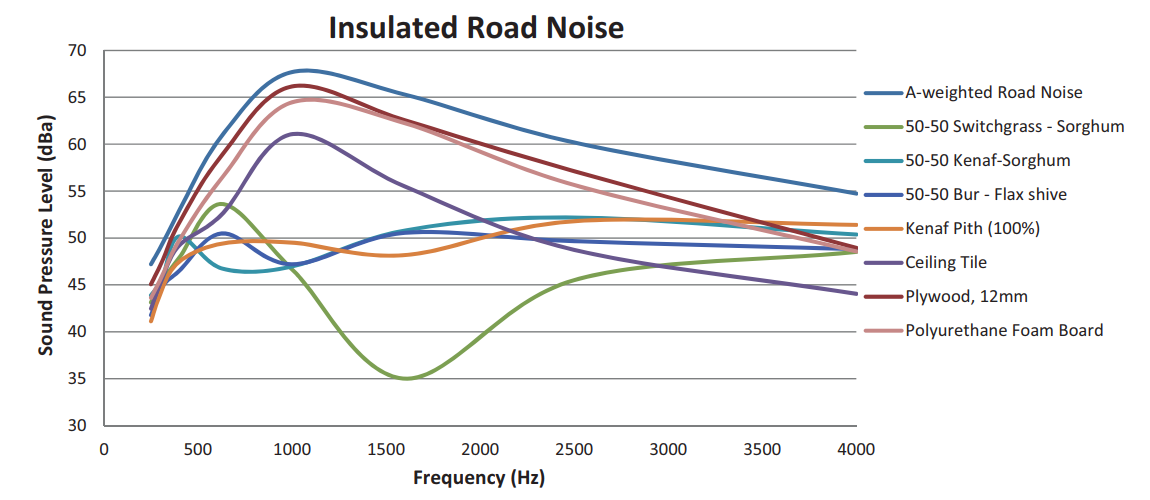
Acoustic absorption of different mycelium based acoustic panels.
Pelletier, M., Holt, G., Wanjura, J., Bayer, E., & McIntyre, G. (2013). An evaluation study of mycelium based acoustic absorbers grown on agricultural by-product substrates. Industrial Crops and Products, 51, 480–485. https://doi.org/10.1016/j.indcrop.2013.09.008
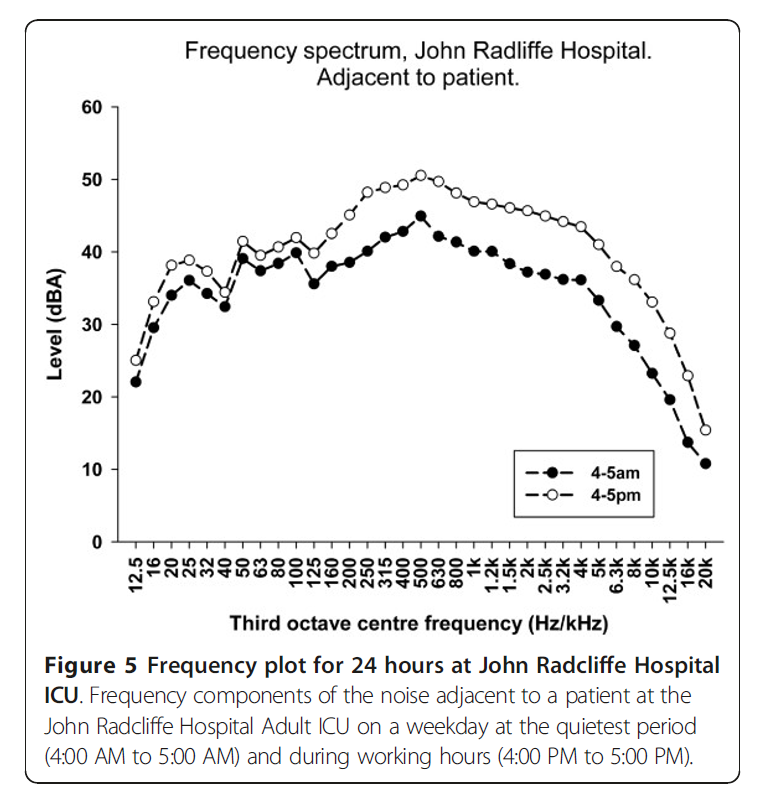
Frequency in patient care units.
Darbyshire, J. L., & Young, J. D. (2013). An investigation of sound levels on intensive care units with reference to the WHO guidelines. Critical Care, 17(5). https://doi.org/10.1186/cc12870
Other useful fungi applications








Various useful fungi applications